
First Biological Law Second Biological Law Third Biological Law Fourth Biological Law Fifth Biological Law
THE FIVE BIOLOGICAL LAWS OF THE NEW MEDICINE
THE FIRST BIOLOGICAL LAW (“The Iron Rule of Cancer”)
In GNM terms, a DHS is an emotionally distressing event that we could not anticipate and for which we were not prepared. From a biological point of view “unexpected” implies that unprepared for, the situation could be detrimental for the one who was caught off-guard. In order to support the organism during the unforeseen crisis, a Significant Biological Special Program on stand-by for exactly that conflict is instantly activated. The significance of this meaningful biological program of Nature is to improve the function of the organ so that the individual is in a better position to manage and eventually resolve the conflict. Since the DHS occurs at once in the psyche, in the brain, and on the corresponding organ, we speak in GNM of biological conflicts rather than of psychological conflicts.
Since human beings are capable of symbolic thought, we are able to experience biological conflicts also in a figurative sense. For us, an attack conflict can be brought on by an offending remark, a territorial loss conflict with an unwanted move, a starvation conflict through the loss of income, a sexual conflict when our partner is “mating” with someone else, a self-devaluation conflict because of abuse, or a death-fright conflict through the shock of a cancer diagnosis.
In GNM, the PSYCHE is regarded as an integral part of the human biology. It is the “organ”, so to speak, that inherently recognizes dangers. At the very instance of a DHS, the psyche associates with the event a specific biological conflict theme such as “anger in the territory”, “worries in the nest”, “abandonment by the pack”, “separation from a mate”, “loss of an offspring”, and so forth. This association happens in a split second and entirely on a subliminal level. Thus, it is the subconscious reading and subjective assessment of the conflict situation that determines which Biological Special Program will be activated. Yet, how exactly the subconscious mind perceived the particular conflict is only revealed when the physical symptoms arise. Whether a person gets a sore throat, comes down with a cold, has diarrhea, develops a skin condition or a certain cancer is therefore dependent on how the conflict was experienced when the DHS occurred. NOTE: We can also suffer a conflict with or on behalf of someone else.
It goes without saying that our past experiences, our social and cultural conditioning, our values, our beliefs, our knowledge, our expectations, our vulnerabilities, our fears, and other factors contribute greatly to the perception of a conflict situation. Psychological aspects can undoubtedly create a predisposition for a biological conflict. However, independent of a DHS they are not able to activate a Biological Special Program, because, like all species, we humans respond to unexpected distress biologically rather than intellectually or on a solely psychological level.
When the DHS occurs, the conflict is registered on all three levels at once.
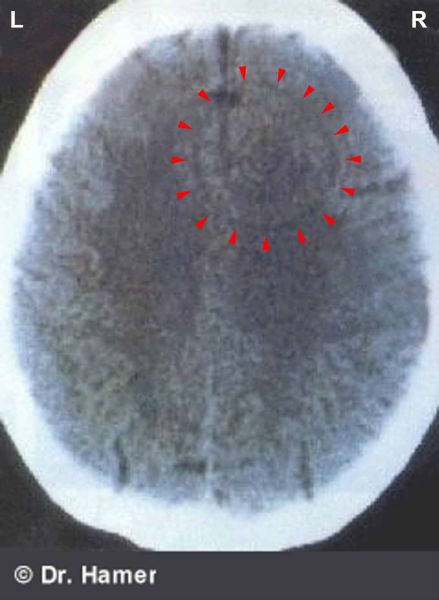
BRAIN LEVEL: At the moment of the DHS, the conflict shock impacts in a specific, predetermined area in the brain. On a brain CT (brain computer tomogram) the impact is visible as a set of sharp concentric rings or as a semicircle, depending on the location. In GNM, such a ring configuration is called a Hamer Focus or HH (from German: Hamerscher Herd). The term was originally coined by Dr. Hamer's opponents, who mockingly named these structures “dubious Hamer Foci”.
Before Dr. Hamer discovered these ring structures, radiologists disregarded them as artifacts created by a glitch in the machine. In 1989, Dr. Hamer asked Siemens, a manufacturer of computer tomography equipment, to explain which criteria must be fulfilled to exclude a ring artifact. An official Siemens document confirms that these target rings cannot be artifacts, because even when the tomography is repeated and taken from different angles, the same configuration always appears in the same location. Moreover, during the course of an SBS, the Hamer Focus changes from a sharp ring configuration (conflict-active phase) to an edematous ring structure (in PCL-A) to an HH with neuroglia (in PCL-B). Hence, if several Biological Special Programs run concurrently, more than one Hamer Focus is visible on a brain scan, and this often in different phases.
In the practice of GNM, a brain CT is the ultimate diagnostic tool. A thorough brain scan analysis allows drawing reliable conclusions as to the nature of the DHS, the intensity of the conflict, which organ is affected, whether the SBS is in the conflict-active phase or in the healing phase, and what healing symptoms have to be expected once the conflict has been resolved. The Hamer Foci (we could also call them “conflict markers”) are the exact proof that the psyche communicates with all organs of the body via the brain as the control station from where the Significant Biological Special Programs are coordinated.
The Psyche – Brain – Organ Relation
Head Brain and “Organ Brain”
This meaningful interplay between the psyche, the brain, and the body has been in place for millions of years. Originally, these biological survival programs were directed from the “organ brain” (plants still possess such an organ brain; they suffer biological conflicts, for example, through the exposure to acid rain). With the growing complexity of life forms, however, a “head brain” (the master controller) developed from where each Biological Special Program is coordinated. The transfer from the “organ brain” to the “head brain” explains why, in line with evolutionary reasoning, the control centers in the brain are arranged in the same order as the organs in the body. The cells of the human body are quasi the “primeval brain” with the cell nuclei as the micro-computers controlled from the head brain as the supervising home station. The head brain and the cell-“brains” are neurally connected. They therefore vibrate at the same frequency.
ORGAN LEVEL: With the impact of the conflict in the correlating brain relay, the DHS is instantly communicated to the corresponding organ and the Biological Special Program is set into motion.
BIOLOGICAL HANDEDNESS
In the practical application of GNM it is of utmost importance to ascertain a person’s biological handedness, because the handedness determines whether the conflict impacts on the right or left side of the brain and whether a symptom (skin rash, muscle weakness, rheumatic pain, breast cancer) occurs on the right or left side of the body, taking into account the cross-over correlation from the brain to the organ (the brain-organ relation is always unequivocal).
In addition, the right and left sides of the body are assigned to mother/child and partner-related conflicts (see nest-worry conflicts, separation conflicts, hearing conflicts, attack conflicts, self-devaluation conflicts). A partner includes a person’s spouse, siblings, relatives, colleagues, business partners, neighbors, schoolmates, friends, or foes. For a man his child is associated with his mother/child-side when he is raising the child or when his father feelings are very strong, otherwise, the child is considered a partner. For a child, his/her father is the first “partner”. By the same token, the mother can be perceived as a partner when the child grew up with the grandparents or when the mother-child relationship has deteriorated. If an adult cares for a sick father like for a child, the father is most likely associated with the mother/child side. A pet can be perceived as a child or as a friend (partner). A conflict evoked by a partner, for example a separation conflict, is mother-related if the subconscious mind makes a connection with the mother (“This also happened to my mother”). What ultimately counts is with whom the conflict is associated at the moment of the DHS (compare with localized conflicts).
An easy way to establish the biological handedness is the clapping test – clapping the hands like applauding in the theatre. The hand that is on top is the leading hand and tells whether a person is right-handed or left-handed. Also, right-handers start walking with the right foot, left-handers with the left foot. Left-handers are usually ambidextrous.
The principle of laterality: A right-handed person responds to a conflict with his/her mother or child with the left side of the body and to a conflict with a partner with the right side. With left-handed people it is reversed. Hence, a left-handed person associates a conflict with his/her mother or child with the right side of the body and a conflict with a partner with the left side. This rule applies to all organs controlled from the cerebellum, cerebral medulla, and cerebral cortex (except for the temporal lobes, glucose center, and brain relays of the thyroid ducts and pharyngeal ducts – see principle of gender, laterality, and hormone status below). NOTE: With organs controlled from the brainstem, a person’s handedness is irrelevant.
The biological right and left-handedness proves that physical symptoms arising from a DHS originate from a biological conflict. Standard medical theories claiming that “diseases” are caused by a “weak immune system”, a wrong diet, faulty genes, pathogenic microbes, geopathic stress, or by beliefs (“Beliefs can make you sick” – Bruce Lipton) are not able to explain why a specific condition such as dermatitis, joint pain, muscle paralysis, or certain cancers develop on the right or left side of the body (or on both). From a strictly psychological point of view, this makes no sense either.
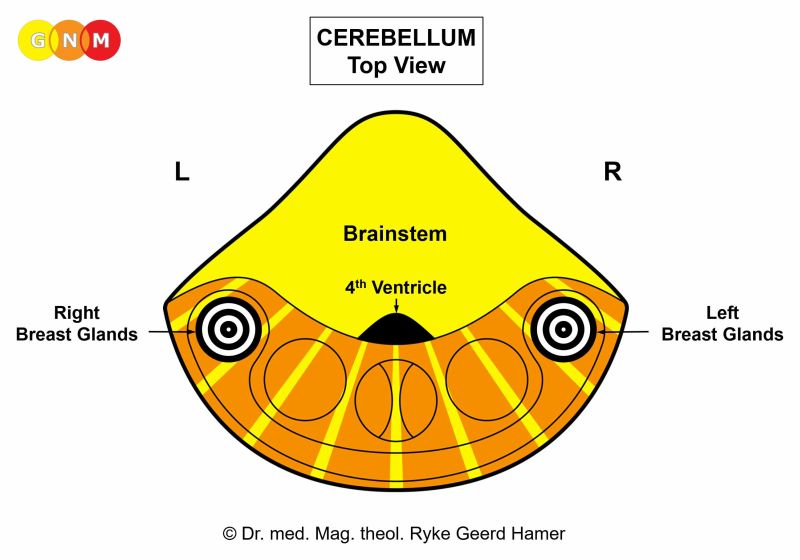
A central or para-central conflict refers to a DHS that is experienced simultaneously as a mother/child and partner-related conflict involving both sides of the body. For example, if a right-handed woman perceives her grown-up child predominantly as a partner, the symptoms (skin rash, rheumatic pain, joint pain) appear mostly on the right side (her partner-side). In this case, the center of the Hamer Focus is located on the left brain hemisphere (para-centrally). With a conflict linked to a paired organ such as the breasts, the nest-worry conflict impacts in both breast gland relays, affecting the right and left breast.
A localized conflict affects the area of the body that was associated with the conflict. For example, a hit on the right shoulder (attack conflict) affects the relevant area of the corium skin, independent of the mother/child and partner-side.
A generalized conflict relates to a DHS that affects a person as a whole. Subsequently, the symptoms occur on both sides of the body. Generalized conflicts (separation conflicts, self-devaluation conflicts) occur predominantly in children and the elderly.
THE PRINCIPLE OF GENDER, LATERALITY, AND HORMONE STATUS
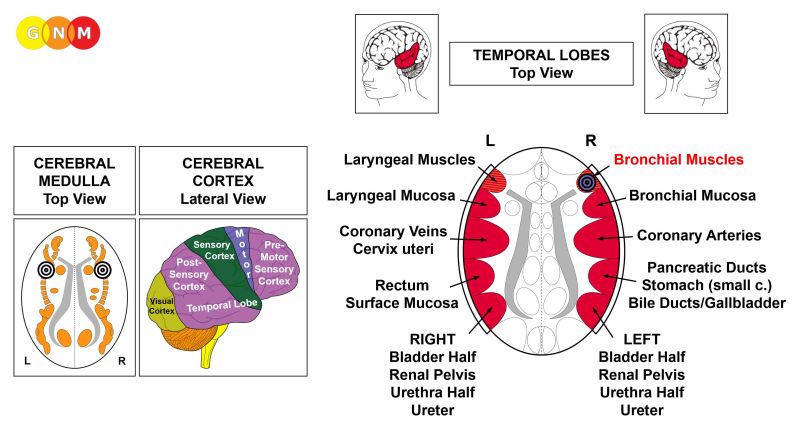
With organs and tissues controlled from the cerebral cortex, specifically from the temporal lobes (bronchial muscles, bronchial mucosa, laryngeal muscles, laryngeal mucosa, coronary arteries, coronary veins, cervix uteri, small curvature of the stomach, bile ducts, gallbladder, pancreatic ducts, rectum surface mucosa, renal pelvis, ureters, bladder, and urethra), the pre-motor sensory cortex (thyroid ducts, pharyngeal ducts), and the glucose center (alpha islet cells and beta islet cells of the pancreas), we have to take into account a person's gender, handedness, and hormone status. Whether the conflict is mother/child or partner-related is of no consequence.
A change of the hormone status alters a person’s biological identity and consequently the way in which conflicts are perceived. For example: When a woman is postmenopausal, her testosterone level is relatively higher than her estrogen level; she experiences therefore conflicts just like a male. In females, the estrogen level decreases during pregnancy and nursing, after menopause, with an ovarian necrosis in both ovaries, when both ovaries have been removed, and due to estrogen-lowering medication or contraceptives (progesterone in birth control pills suppresses the production of estrogen). In males, the testosterone level decreases in elderly men, with a testicular necrosis in both testicles, when both testicles have been removed, and due to testosterone-lowering medication. After radiation or chemo treatments the production of sexual hormones drops altogether.
With the impact of a DHS in the female conflict area, the estrogen level decreases proportionally to the degree of conflict activity. Conversely, with an impact in the male conflict area, the testosterone level goes down. In GNM we call this a conflict-related hormonal imbalance.
In the practice of GNM, the application of the principle of gender, laterality, and hormone status allows establishing with certainty the type of conflict that causes the symptoms on the corresponding organ.
Let’s take as an example the scenarios of a male territorial fear conflict and a female scare-fright conflict related to the bronchial mucosa and the laryngeal mucosa (controlled from the temporal lobes).
| |||||||||||||||||||||||||||||||||||||||||||||
















THE SECOND BIOLOGICAL LAW
 Normotonia, sympathicotonia, and vagotonia are terms that relate to the autonomic nervous system which controls vegetative functions such as sweating, respiration, digestion, excretion, constriction of blood vessels, and the heartbeat.
Normotonia indicates a balanced day-night-rhythm where sympathicotonia alternates with vagotonia. During the day, the organism is in a normal sympathicotonic state of stress (“fight or take flight”), during sleep in a normal vagotonic state of rest (“rest and digest”). The sympathicotonic phase lasts roughly from 4 am in the morning to 8 pm at night.
The Second Biological Law shows that every Biological Special Program proceeds in this two-phase pattern. In GNM, the change of the vegetative rhythm is an important diagnostic criterion for establishing whether a person is in the conflict-active phase or in the healing phase.
THE CONFLICT-ACTIVE PHASE (CA-Phase)
When the DHS occurs, the normal day-night-rhythm is instantly interrupted and the autonomic nervous system switches into lasting sympathicotonia and a prolonged state of stress with nervous restlessness, a fast heartbeat, elevated blood pressure, slow digestion, frequent urination, and little appetite. Since the blood vessels are constricted during stress, typical signs of conflict activity are cold hands, cold sweats, and the shivers. We therefore call the conflict-active phase also the COLD phase.
The PSYCHE is in a compulsive thinking mode. The constant dwelling over the conflict causes sleep disturbances (waking up shortly after falling asleep, usually around 3 o’clock in the morning). The extra waking hours and the total focus on the conflict serve to find a resolution to the conflict as soon as possible.
The psyche, the brain, and the corresponding organ are three levels
of ONE unified organism that always work in synchronicity.
BRAIN LEVEL: The Biological Special Program is directed from the brain relay that corresponds to the specific conflict as well as to the correlating organ.
ORGAN LEVEL: In unison with the psyche and the autonomic nervous system, the conflict-related organ responds with physical changes that serve the biological purpose to improve the function of the organ so that the individual is in a better position to cope with the conflict.
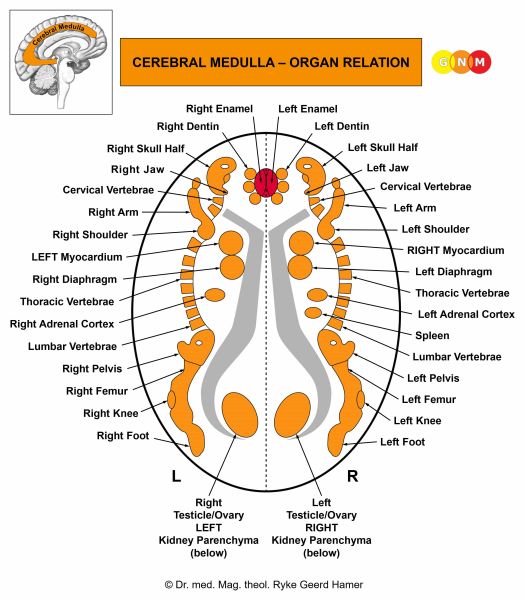
 If more tissue is required to facilitate a conflict resolution, the corresponding organ generates cell proliferation during the conflict-active phase. This process applies to all organs and tissues that are controlled by the brainstem and the cerebellum such as the lungs, liver, pancreas, colon, thyroid, or breast glands. In embryological terms, these organs derive from the endoderm or from the old mesoderm (see Third Biological Law).
With long-lasting conflict activity, the continuous cell augmentation forms a tumor or cancer. A cancer that originates in glandular tissue such as the breast glands and a tumor that has a secretory quality (see organs of the alimentary canal) are called an adenocarcinoma. Since the additional cells (the “cancer cells”) proliferate proportionally to the degree of conflict activity, they have the ability to multiply very quickly (they also differ genetically from the original cells). Conventional medicine considers the fast cell mitosis erroneously as “abnormal” and as “cells growing out of control”. If the rate of cell division exceeds a certain limit, the tumor is interpreted as “malignant” (based on an academic consensus!). Dr. Hamer's discoveries turn this paradigm completely on its head by demonstrating that “diseases” such as cancer are not, as assumed, malfunctions of an organism but instead Significant Biological Special Programs of Nature designed to support an individual during unexpected distress. His research provides the scientific evidence that cancer cells are in reality specialized cells that actively participate in the function of an organ in order to assist the organism in the event of a biological emergency situation. In lung cancer, for example, the extra cells improve the capacity of the lungs in response to a death-fright conflict, in colon cancer they increase the production of digestive juices to be better able to manage an indigestible morsel conflict, in breast cancer the additional milk-producing cells allow a female to provide more milk for a sick offspring in the event of a nest-worry conflict. In light of the Five Biological Laws and the new understanding of “diseases”, the distinction between “malignant” and “benign” becomes entirely meaningless.
If less tissue is required to facilitate a conflict resolution, the organ or tissue responds with cell loss. This process applies to all organs and tissues that are controlled from the cerebral medulla and the cerebral cortex such as the bones and joints, ovaries, testicles, coronary arteries, coronary veins, cervix uteri, bronchial mucosa, laryngeal mucosa, and epidermis. In embryological terms, these organs derive from the new mesoderm or from the ectoderm (see Third Biological Law).
HANGING CONFLICT
Many of us are living with “hanging conflicts” with little or no symptoms since symptoms in the conflict-active phase are rare. Lasting intense conflict activity, however, drains the body of energy, which could lead to death. Yet, a person can never die of cancer! Those, who don't make it through the conflict-active phase die as a result of energy loss, weight loss, sleep deprivation and, above all, because of the fear of the “disease”, particularly the fear of cancer. With a negative prognosis (“You have six months to live!”), “metastasis”-scares (“The cancer is spreading!”), and highly toxic chemo treatments added to the emotional and mental distress, cancer patients have little chance to survive. Worn out and exhausted, they waste away and eventually die of cachexia.
In GNM, we take the following approach: If an intense conflict cannot be resolved at the time, the objective is to downgrade the conflict by finding partial resolutions. Downgrading a conflict slows down the cell proliferation on the corresponding organ and reduces therefore the size of a tumor that develops during the conflict-active phase. We can live with a hanging conflict and with cancer into old age (for reassurance surgery is an option).
CONFLICTOLYSIS (CL)
Conflicts always originate from real life circumstances, brought on, for instance, by problems with a spouse (separation conflicts), the death of a loved one (loss conflicts), troubles at work or in school (territorial conflicts, self-devaluation conflicts), financial difficulties (starvation conflict, morsel conflicts), worries about a family member (nest-worry conflicts), or concerns about oneself (existence conflicts, death-fright conflicts). Trying to find a practical solution is, therefore, the best as it is most lasting. The loss of a workplace, for example, could be dealt with by picking up an old hobby; constant “territorial anger” with a neighbor might require a move. Sometimes, conflicts resolve themselves, for instance, when life-circumstances change or when other matters gain more priority. On a spiritual level, conflicts we are facing are an invitation to reconsidering our attitude, letting go of anger, viewing the situation from a different angle, trying to see the larger picture, understanding the position of the people involved, and to practicing forgiveness and loving kindness as the true source of healing. From a higher viewpoint, making GNM part of our daily life contributes greatly to our personal growth and development. It is not without reason that the Spanish call the New Medicine La Medicina Sagrada or The Sacred Medicine.
Learning GNM not only allows us to become aware of our individual conflicts as the cause of an ailment, it also puts us into the fortunate position to welcome – free from fear – the healing symptoms.
THE HEALING PHASE (PCL = post-conflictolysis)
With the resolution of the conflict, the autonomic nervous system switches into lasting vagotonia and a prolonged state of rest with fatigue but good appetite. Resting and the desire to eat provide the organism with the necessary energy for healing. If the healing phase is intense, the tiredness could be so overwhelming that one can hardly get out of bed. The need for sleep is particularly strong during the day (in conventional medicine, persistent tiredness is diagnosed as “chronic fatigue syndrome”). Accompanying symptoms are a slow pulse and low blood pressure. During vagotonia, the blood vessels expand causing warm hands and a warm skin. We therefore call the healing phase also the WARM phase.
The PSYCHE is in a state of relief.
ORGAN LEVEL: During the healing phase the affected organ is restored to its normal function.
Tumors that developed in the conflict-active phase such as a lung tumor, colon tumor, liver tumor, prostate tumor, or a tumor in the breast glands immediately stop growing and the extra cells that are no longer required are broken down with the help of microbes (Fourth Biological Law). This applies to all organs controlled from the brainstem and the cerebellum.
Conversely, cellular depletion, for example, in the ovaries, testicles, cervix uteri, bronchial mucosa, milk ducts, or bile ducts is refilled and replenished with new cells (in conventional medicine, the new cells are wrongly regarded as “cancer cells”). This applies to all organs and tissues controlled from the cerebral medulla and the cerebral cortex.
In PCL-A (exudation phase) an edema forms at the site to protect the area that is healing at the time. With water retention as a result of an active abandonment or existence conflict (see the SYNDROME) the retained water is exceedingly stored in the healing area, which enlarges the swelling. Other signs of healing are fever and inflammation because of the increased blood flow into the healing tissue, discharge to expel the by-products of the cell removal process, itching when epithelial tissues such as the skin are affected, and night sweats when fungi and TB bacteria are involved. The swelling and the inflammation can cause considerable pain. The severity of the healing symptoms is determined by the intensity of the preceding conflict-active phase. NOTE: Complications don’t arise from high fever but due to a large brain edema.
BRAIN LEVEL: The impact of the conflict (DHS) in the brain causes a slight damage to the neurons within the specific brain relay. Parallel to the healing of the psyche and the organ, the affected neurons also undergo a restoration process. Like on the organ level, during the first part of the healing phase (PCL-A) water and serous fluid are drawn to the area, creating a brain edema to protect the brain tissue during that period. The extent of the edema is determined by the intensity of the preceding conflict and the size of the Hamer Focus created at the moment of the DHS.
It is the swelling of the brain edema that causes cerebral healing symptoms such as dizziness and headaches. Headaches that occur during PCL-A are dull pressure headaches. Sharp, stabbing headaches, on the other hand, happen after the Epileptoid Crisis (in PCL-B). Once the brain edema has been expelled, the mechanical pulling on the meninges is felt as sharp pain. Migraine headaches start in the healing phase and are most intense during the Epileptoid Crisis (rightfully, migraines were once called “small epilepsy”). They involve predominantly the pre-motor sensory cortex. Conflicts linked to migraines are, for example, powerless conflicts, frontal-fear conflicts, oral conflicts, stink conflicts, or bite conflicts. Typically, the conflict-active phase was short but intense. Recurring migraine attacks are caused by conflict relapses (“Sunday migraines” are triggered by a “Sunday track”).
In general, the brain edema is nothing to worry about. However, a big swelling, usually caused by water retention (the SYNDROME) might create such strong pressure that a person falls into a coma and dies. The same risk exists with multiple brain edemas. Sudden infant death (SIDS or “crib death”) occurs due to large swellings in the brain.
THE EPILEPTOID CRISIS is initiated at the height of the healing phase and takes place simultaneously on all three levels. At the start of the crisis, the entire organism is pulled out of the vagotonic state and the individual is for the time being in a conflict-active state of stress. The reactivation of the conflict generates restlessness, nausea, elevated blood pressure, a raised pulse, cold sweats, and the shivers. The biological purpose of the sympathicotonic surge is to expel the edema that developed both on the organ and in the correlating brain relay (in PCL-A); the expelling of the brain edema is particularly vital as it relieves the brain pressure. The Epi-Crisis is followed by a urinary phase, in which the body eliminates all the excess fluid. If the edema cannot be completely expelled because of the SYNDROME (water retention) or due to conflict relapses, the residual edema remains until the Biological Special Program is complete.
The exact type of Epileptoid Crisis is determined by the nature of the conflict, which organ is affected, and which part of the brain is involved. When a brain edema is in the motor cortex, the crisis manifests as rhythmic convulsions (see epileptic seizure), muscle cramps or spasms; in the sensory or post-sensory cortex, it generates dizzy spells, short disturbances of consciousness or, with an intense conflict, a complete loss of consciousness (“absence”) due to the drop of blood sugar. Some Epi-Crises could be dangerous, especially when the conflict-active phase was long and intense. This applies, for instance, to heart attacks or strokes. The Epileptoid Crisis is a significant biological counter-regulation. Dr. Hamer therefore strongly advises not to take antispasmodic or sedative medication during this period in order not to interrupt this highly critical event. Sedatives administered at that point could cause a person to fall into a coma.
The Epileptoid Crisis usually occurs during periods of rest (weekends, holidays, vacation), in the early morning hours or during sleep when the organism is in deep vagotonia. The extent of the Epileptoid Crisis is determined by the degree of the conflict-active phase. Hence, most of the time the healing crisis is completely harmless and only evident, for instance, as coughing fits, diarrhea attacks, nose bleeds, or as “the cold days” (chills) and nervousness.
Passing the Epileptoid Crisis is like turning a corner. Now, the organism enters the second part of the healing phase, or PCL-B (scarification phase). Scarring occurs predominantly through the production of collagen manufactured by specialized cells, called fibroblasts, located in the connective tissue around the healing area. By the end of the Biological Special Program, the original function of the organ is restored and the day-night-rhythm returns to normotonia.
BRAIN LEVEL: After the brain edema has been pressed out, glial cells proliferate at the site to finish the healing process on the cerebral level. Neuroglia (“glia” comes from the Latin word for “glue”) is brain connective tissue that insulates and supports neurons. Only 10% of the brain consists of nerve cells; 90% is made up of glial cells, which indicates their importance. A major distinction between the two types of brain cells is that neurons do not divide by mitosis, while glial cells have the ability to multiply. Similar to the role of connective tissue in wound healing, the function of neuroglia is to repair brain damage, for example after a brain injury or brain surgery. Glial cells also help to restore the area in the brain that received the impact of a DHS. Intense conflict activity as well as the brain edema (in PCL-A) stretch the synapses (junction between nerve cells) putting stress on the insulation around neurons. During the healing phase, glial cells mend the neural sheath by forming an additional insulating layer. This repair work is crucial to ensure a normal function of the organ that is controlled from that particular brain relay.
In conventional medicine, the natural buildup of neuroglia is wrongly believed to be a “brain tumor”, termed “glioma”, “glioblastoma”, or “astrocytoma” (referring to the star-shaped form of glial cells). The classification of brain tumors (grade 1 to 4) is based on the density of glial cells; grade 4 is considered the “most aggressive” with the propensity to “spread throughout the brain”. If more than one “tumor” is found in the brain, the diagnosis reads: “multiple brain metastases” (which usually triggers instantly a new DHS!).
Dr. Hamer demonstrated already in the early 1980s that so-called brain tumors are not cancers but instead an indication that a natural healing process is taking place in the brain parallel to the healing on the corresponding organ (symptoms on the related organ might not be noticed, particularly, if there is no water retention which would increase the swelling, causing pain). In GNM terms, a brain edema and a “brain tumor” is a Hamer Focus in different phases of a Biological Special Program.
The surgical removal of a tumor does not stop the healing process. This is why “brain tumors” come back, unless the mutilating surgery went far into the healthy tissue. After the excision, the surgical cavity forms a cyst that becomes over-inflated by the surrounding edema. Measures such as inserting a shunt into the brain to drain the extra fluid put additional stress on the brain.
A brain cyst also forms when the healing phase is repeatedly interrupted by conflict relapses. With the constant alteration between conflict activity and healing, the brain edema alternatively contracts and expands. Due to the “accordion effect”, the brain tissue becomes rigid and inflexible. At one point, the tissue ruptures resulting in the formation of a fluid-filled cyst. The tearing might cause brain bleeding (erroneously believed to be caused by a stroke). Chemo treatments have the same effect. With each chemo regimen, the healing process comes abruptly to a stop and the brain edema gets smaller; after the treatments, healing continues and the edema starts to grow again. Radiation treatments also compromise healing. Brain tissue that has been irradiated loses the elasticity required when new brain edemas form in the course of future healing phases.
HANGING HEALING
When we experience a DHS, our mind is in a state of acute awareness. Highly alert, our subconscious picks up all components considered as relevant in association with the conflict situation. In GNM, we call the imprints that remain in the aftermath of a DHS tracks (with reference to train tracks on which a train travels). Tracks are, for example, the location where the conflict took place, a person or pet that was involved, the taste of a particular food, specific sounds or noises, the weather condition, a certain scent (perfume, flowers), certain words, a voice, a gesture, and so forth. Setting on a track can be highly emotional. In fact, feelings such as fear or distress itself can become a track. Other tracks stored in the biological memory are more subtle, for instance, a food ingredient or certain pollen. The biological purpose of the tracks is to function as a warning signal in order to avoid experiencing the same conflict a second time. In the wild, these alarm signals are vital for survival.
If we are in the healing phase and suddenly encounter a track, either through direct contact or by association, the original conflict is instantly reactivated. Each conflict relapse interrupts and therefore prolongs the healing process – on the correlating organ as well as in the corresponding brain relay – leading to a chronic condition. Persistent skin conditions (dermatitis, psoriasis), arthritis, Crohn’s disease, Parkinson’s, “chronic fatigue syndrome” (prolonged vagotonia), or constant low blood pressure are examples of a hanging healing. Like with a healing wound that is torn open again and again, with conflict relapses the affected organ heals only very slowly. This is why we should try to resolve a conflict as soon as possible. NOTE: Being constantly on a conflict track causes a hanging conflict.
Tracks also have to be taken into consideration when we are dealing with recurring conditions such as recurring colds, skin rashes, diarrhea, hemorrhoids, “infections”, or recurring cancers. Returning symptoms (flare-ups) are always a sign that certain tracks associated with a particular conflict are still of importance, although the healing phase has been completed. In this case, setting on a track triggers a quick replay of the Biological Special Program with the conflict-related healing symptoms, including symptoms of the Epileptoid Crisis (coughing fits, asthma attack, migraine attack) following right away. Based on GNM, so-called “allergies” are therefore always manifestations of tracks.
In light of the significance of tracks, so-called “allergens” (pet dander, pollen, foods) are important warning signals. Contrary to the standard theory, antibodies do not, as assumed, fight the allergen (based on the construct of an “immune system”) but put the organism on the alert by reactivating the conflict. For this reason, white blood cells start to produce “antibodies” (really a misnomer) as soon as the DHS occurs. Their sole purpose is to set off an alarm (the organ related symptoms) in the event of an encounter with a conflict track. This is why an allergy test is “positive” if the applied antigen, for example a certain food, happens to be a track.
GNM is able to explain why one and the same allergen, for instance a milk-track, causes different symptoms in different people. It is the actual allergy symptom (a runny nose, red and itchy eyes, coughing, diarrhea, or a skin rash) that reveals the nature of the original conflict. Hence, we are not allergic to specific foods, cleaning agents, cosmetics, metals (jewelry made of gold or silver), mold, or dust mites, but rather to what we associate with it! We can therefore also be “allergic” to a certain person, a specific location, or a particular piece of music.
In the practical application of GNM identifying the track(s) is of utmost importance, because only then will an “allergy” stop reoccurring. Recognizing that the conflict has been resolved and bringing into awareness that the tracks are no longer a “danger” and that the extended tracks are now irrelevant provides the ultimate chance to complete the healing of chronic conditions. NOTE: Talking about the DHS can reopen the conflict wound. The true GNM therapist will therefore proceed with caution and care.
|









THE THIRD BIOLOGICAL LAW (“The Ontogenetic System of Tumors”)
Dr. Hamer's medical research is firmly anchored in the science of embryology. Taking into account the development of the fetus (ontogenesis) he discovered that the correlation between the psyche, the brain, and the organs is closely connected to the three embryonic germ layers (endoderm, mesoderm, ectoderm) from which all organs of the human body originate. The Third Biological Law shows that the location of the Hamer Focus in the brain as well as the cell proliferation or cell loss following a DHS are not accidental but part of a meaningful biological system inherent in every living organism. The Biological Special Programs of Nature are encoded in every human cell and thus inscribed in the DNA, the carrier of genetic information (see GNM Article “Understanding Genetic Diseases”).
Through analyzing and comparing thousands of brain scans Dr. Hamer found that organs originating from the same embryonic germ layer are controlled from the same part of the brain.
Some organs, notably the colon, originate only from one embryonic germ layer. Others such as the kidneys are made up of tissues that derive from all three germ layers. Over time, the tissues merged for functional purposes and formed one organ or organ system (reproductive system, digestive system, renal system, respiratory system, circulatory system). This explains why parts of one organ have their control centers in different areas of the brain. In the body, organs of the same germ layer origin, for instance, the laryngeal mucosa, cervix uteri, coronary veins, rectum surface mucosa, and bladder mucosa are not always grouped together. In the brain, however, their control centers are positioned side by side, in perfect order.
Each of the three embryonic germ layers corresponds to very specific biological conflicts that date back to the time when the life-threatening crisis (existence conflict, starvation conflict, water conflict, territorial loss conflict) first occurred. Hence, certain conflict themes belong to a particular evolutionary period.
|

THE FOURTH BIOLOGICAL LAW
For the first 2.5 billion years, microbes were the only organisms inhabiting the earth. Gradually, they populated other life forms, including plants, animals, and humans. It is estimated that the number of microbial cells residing in the human body (known as the “human microbiome”) outnumbers the body cells almost 4 to 1. Owing to their symbiotic relationship with the human organism and their vital role in maintaining the body tissues, microbes have become indispensable for our survival.
The theory that certain “diseases” are caused by “pathogenic microbes” is one of the most persistent doctrines of modern medicine. This general conception is largely attributable to the fact that microbes are present at the site of a “diseased” organ. And since the activity of microbes is accompanied by swelling, fever, inflammation, pus, discharge, and pain, microbes are believed to be the cause of “infectious diseases”. Similar to the idea that an “abnormal” growth of cancer cells leads to the development of a “malignant” tumor, it is wrongly assumed that microbes growing beyond their normal ranges (see immune system theory) results in virulent “infections”.
Microbes don’t cause diseases but play instead a vital role during the healing phase.
The Fourth Biological Law shows that so-called “infectious diseases” occur exclusively in the second phase of a Biological Special Program, where the organism uses the microbes to optimize healing. During their activities microbes require a warm environment, hence, the development of an inflammation and fever. Microbes also need an acidic milieu, which is suitably provided through the vagotonic state that is dominant in every healing phase. The onset of an “infection” is therefore not, as presumed, brought on by an imbalanced pH level (a “wrong diet”) but rather by the transition from the conflict-active phase into the healing phase.
White blood cells such as leucocytes and lymphocytes support the microbial work. Governed by images of a biological warfare raging within the human organism, conventional medicine interprets a rise in white blood cells (“killer cells”) as an “immune response” aimed at “attacking” and “fighting the infection”. In light of the Fourth Biological Law, the academic construct of an “immune system”, envisioned as a “defense system” against microbes (and cancer cells), becomes entirely meaningless; in fact, the term “infection” itself becomes obsolete. The invention of “autoimmune diseases”, in which the immune system apparently attacks the body's own tissue, shows how a scientific culture can become blinded by its own beliefs.
Diseases are not contagious!
Based on the two-phase pattern of every SBS (Second Biological Law), “infections” cannot be transmitted to another person since the symptoms (discharge, inflammation, fever) are already healing symptoms. Moreover, a DHS that activates a Biological Special Program is a highly individual conflict experience. If two or more people happen to have the same symptoms, for example, a cold, diarrhea, or a stomach flu, this means that all of them are in the healing phase of the same type of conflict (stink conflict, indigestible morsel conflict, territorial anger conflict) that took place, let’s say, in school, at home, or at work. The idea that everyone had a “weak immune system” just at that time is rather far-fetched. The same holds true for epidemics which are the result of conflicts affecting large populations (attack conflicts, territorial fear conflicts, death-fright conflicts). This was the case, for instance, with the Great Plague, the Spanish Flu, and the lung tuberculosis epidemic after World War I. Nowadays, such collective conflict shocks are easily evoked through frightening media reports (threats of an economic collapse, threats of a global war, threats of terrorist attacks, threats of a “deadly virus”). The ensuing pneumonia outbreak (termed SARS, the swine flu, and so forth) is a self-fulfilling prophecy.
The Ontogenetic System of Microbes
Controlled from the brain, microbes work in a well-planned manner. In normotonia and in the conflict-active phase microbes are dormant, but as soon as the conflict is resolved they start the work assigned to them.
| |||||||||||||||||||||||||






THE FIFTH BIOLOGICAL LAW - THE QUINTESSENCE
| |||||||||||||||||||||




{kind=link}
{kind=link}