
PANCREAS
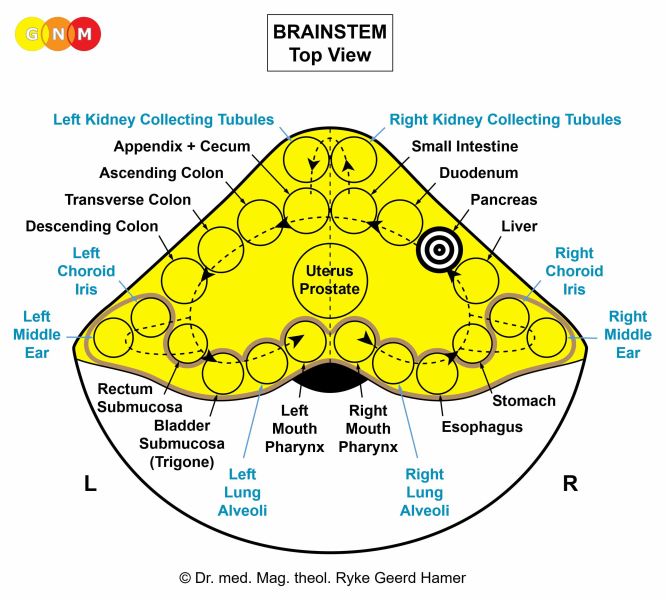
 DEVELOPMENT AND FUNCTION OF THE PANCREAS GLAND: The pancreas is a tube-shaped organ located in the back of the abdomen behind the stomach. The head of the pancreas lies within the curvature of the duodenum. The pancreas gland produces hormones (hormonal quality), including insulin and glucagon, and secretes pancreatic juices (secretory quality) that are released into the small intestine to assist the digestion of food. The pancreas gland consists of intestinal cylinder epithelium, originates from the endoderm and is therefore controlled from the brainstem.
BIOLOGICAL CONFLICT: The biological conflict linked to the pancreas gland is an “indigestible morsel conflict” (see also stomach, duodenum, small intestine, and colon). The conflict is typically brought on by arguments with family members, for instance, over an “inheritance morsel”, a “property morsel”, or a “money morsel” and by insults or accusations that are hard to digest.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the pancreas gland proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to enhance the secretion of pancreatic juices so that the morsel can be better digested. With prolonged conflict activity (hanging conflict) a cauliflower-shaped growth (secretory type), referred to as a pancreatic cancer, develops as a result of the continuing cell augmentation (compare with “pancreatic cancer” related to the pancreatic ducts). If the rate of cell division exceeds a certain limit, conventional medicine considers the cancer as “malignant”; below that limit, the growth is regarded as “benign” or diagnosed as a polyp (see also healing phase).
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. Healing symptoms are indigestion, abdominal pain because of the swelling in the pancreas, and night sweats. The extent of the symptoms is determined by the degree and duration of the conflict-active phase. Water retention due to the SYNDROME increases the swelling considerably. With an inflammation the condition is called pancreatitis (compare with pancreatitis related to the pancreatic ducts).
A prolonged decomposing process (hanging healing) due to continual conflict relapses leaves caverns in the pancreas (see also lung caverns, liver caverns, breast gland caverns). The loss of pancreas tissue results in an inability to produce pancreatic fluids and thus to digest food properly, causing persistent flatulence and diarrhea. However, the deficiency can be supplemented with digestive enzymes (lipase, protease, amylase) and enzyme-rich food.
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells remain without further cell division. Eventually, the growth becomes encapsulated with connective tissue. In conventional medicine, this is usually diagnosed as a pancreas polyp or as a “benign cancer” (see also conflict-active phase). In case of the pancreas gland, the cells that could not be removed keep producing digestive juices resulting in a permanent overproduction of pancreatic fluid (see also thyroid gland, parathyroid glands, adrenal gland, prostate gland).
|

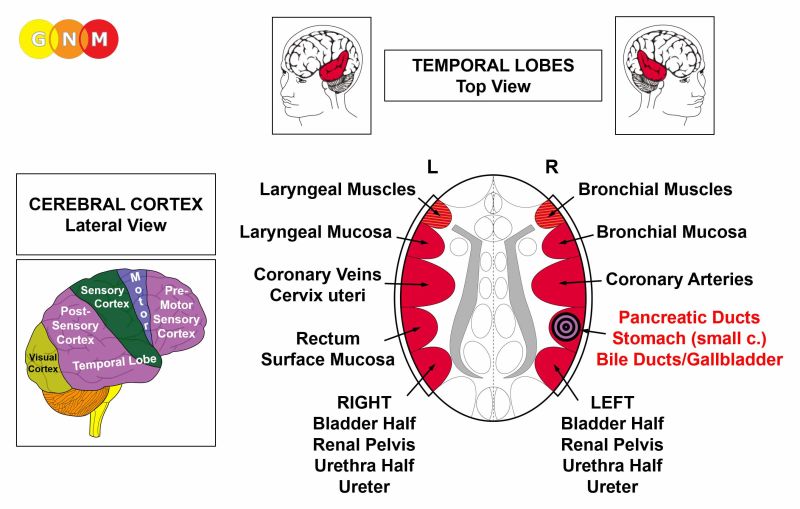
 DEVELOPMENT AND FUNCTION OF THE PANCREATIC DUCTS: The main pancreatic duct connects the pancreas with the small intestine. Its main function is to carry the pancreatic juices produced in the pancreas gland into the duodenum, the first section of the small intestine. The lining of the pancreatic ducts, including its many small branches, consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the pancreatic ducts is a male territorial anger conflict (fight in the territory) or a female identity conflict, depending on a person’s gender, laterality, and hormone status (see also Aggressive Constellation).
A territorial anger relates to anger in the environment and places which one considers as his or her domain – literally or figuratively. Typical territorial anger conflicts are disputes at home, feuds at the workplace, anger at school, in kindergarten, at the playground, in a seniors or nursing home, or in the hospital; also in the extended “territory” such as in the village, town, or country where one lives. Battles over a land or property, annoying noise in the house or neighborhood, a fight over a parking place or over a toy, are other examples of what can provoke a territorial anger conflict.
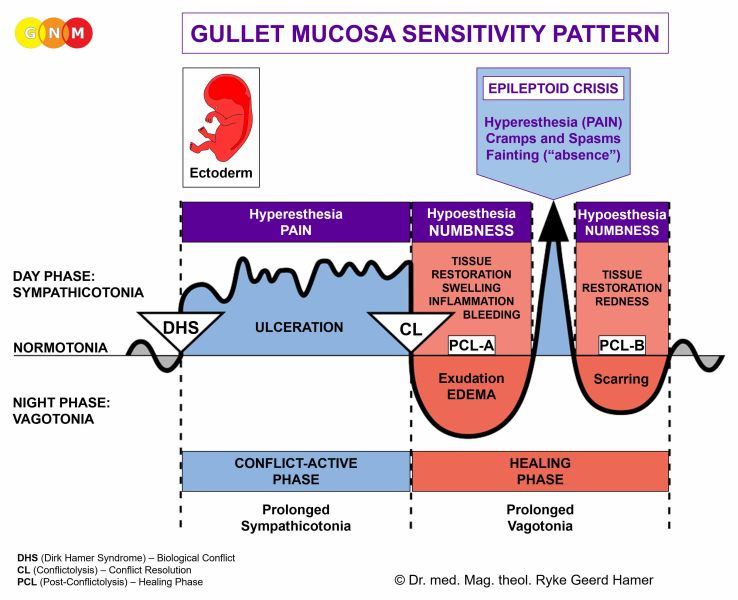
CONFLICT-ACTIVE PHASE: ulceration in the lining of the pancreatic ducts proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the ducts in order to increase the flow of pancreatic fluids. The improved metabolism provides the individual with more energy to resolve the conflict. Depending on the intensity of the territorial anger conflict, the ulceration affects the main duct and/or its small branches. Symptom: mild to severe pain.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation. In conventional medicine, this is usually diagnosed as a “pancreatic cancer” (compare with pancreatic cancer related to the pancreas gland). According to the Five Biological Laws, the new cells cannot be regarded as “cancer cells” since the cell increase is, in reality, a replenishing process.
Healing symptoms are swelling due to the edema (fluid accumulation), indigestion, a fatty stool, and abdominal pain, which could last throughout the entire healing phase (in PCL-A and PCL-B the pain is not of a sensory nature but pressure pain). The pancreatic enzymes (amylase) in the blood serum are elevated. The extent of the symptoms is determined by the intensity and duration of the conflict-active phase. Pancreatitis occurs when healing is accompanied by an inflammation (compare with pancreatitis related to the pancreas gland). With water retention due to the SYNDROME, the enlarged swelling might occlude the duct(s) leading potentially to serious complications.
The Epileptoid Crisis manifests as acute sharp pain and cramps or spasms (pancreatic colic) if the surrounding striated muscles undergo the Epileptoid Crisis at the same time. In PCL-B, the pancreatic ducts open and the function of the organ slowly returns to normal.
|

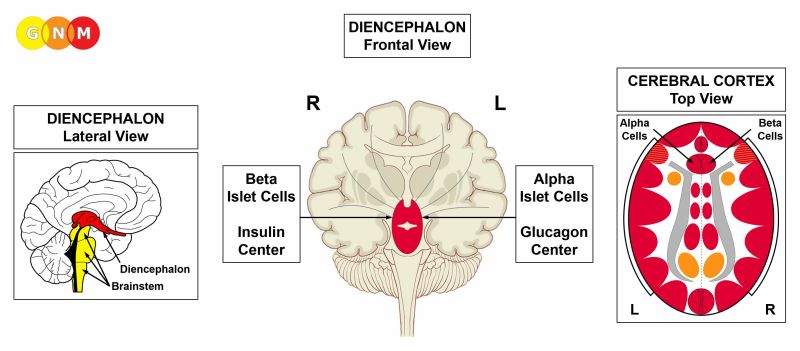
 DEVELOPMENT AND FUNCTION OF THE ISLET CELLS: Embedded in the pancreas gland are cell clusters called the islets of Langerhans that play a significant role in the regulation of blood sugar (glucose). The alpha islet cells secrete glucagon, a hormone that stimulates the liver to convert glycogen to glucose causing an increase of blood sugar. Insulin, produced by the beta islet cells, helps to convert blood sugar into energy by delivering glucose into the body cells. Insulin, therefore, decreases the blood sugar level. The alpha and beta islet cells originate from the ectoderm and are controlled from the diencephalon.
ALPHA ISLET CELLS
BIOLOGICAL CONFLICT: The biological conflict linked to the alpha islet cells is a female fear-disgust conflict or a male resistance conflict, depending on a person’s gender, laterality, and hormone status.
A fear-disgust conflict is a fright coupled with disgust regarding a situation or a person. The conflict can be brought on, for example, by revolting sexual experiences (sexual abuse, unwanted sexual practices, violent sex) or distress involving blood, feces, urine, or vomit. Being frightened of a drunk family member could provoke a fear-disgust conflict with the smell of alcohol as a potential track. Children suffer the conflict when they have to eat “disgusting” food.
CONFLICT-ACTIVE PHASE: During the conflict-active phase the function of the alpha islet cells is reduced. The decrease of glucagon production causes hypoglycemia.
Symptoms of hypoglycemia are nausea, dizziness, fainting (which explains why some people pass out when they see blood), trembling and a fluttering heartbeat due to the glucose deficiency in the muscles, including the heart muscle. Typical for a low blood sugar is a craving for sugar and sweets, which serves the purpose to balance the blood sugar level. The steady over-eating leads to weight gain and obesity (compare with obesity related to water retention). Because of the regular intake of sugar-rich foods, hypoglycemia usually goes unnoticed.
HEALING PHASE: During the first part of the healing phase, in PCL-A, the glucose level slowly rises to a normal level. However, for the period of the Epileptoid Crisis, when the conflict-active symptoms are reactivated, the blood sugar drops temporarily. Acute hypoglycemia (hypoglycemic shock) is a medical emergency! In PCL-B, the blood sugar level increases above the normal range showing the symptoms of diabetes (compare with beta islet cells-related diabetes in the conflict-active phase; see also diabetes insipidus related to the kidneys). At the end of the healing phase, the blood sugar level is back to normal.
With continuous conflict relapses (hanging healing) diabetes becomes chronic. In this case, insulin is still produced but is not utilized for carrying glucose to the body cells (compare with beta islet cells-related diabetes with no insulin production). This is called insulin resistance and categorized as type 2 diabetes, also referred to as adult-onset diabetes (compare with type 1 diabetes or juvenile diabetes).
It has been observed that most people with “type 2 diabetes” are overweight. Being overweight or obese is therefore assumed to be a risk factor for developing diabetes. Based on the GNM knowledge, namely that hypoglycemia and diabetes are two conditions of the same Biological Special Program, we learn to understand that so-called “type 2 diabetes” (in PCL-B) is not caused but rather preceded by hypoglycemia.
BETA ISLET CELLS
BIOLOGICAL CONFLICT: The biological conflict linked to the beta islet cells is a male resistance conflict or a female fear-disgust conflict, depending on a person’s gender, laterality, and hormone status.
A resistance conflict is a strong opposition against a person (parent, stepparent, sibling, relative, spouse, teacher, colleague, supervisor, doctor), against a situation (at work, at home, at school, in a relationship), against an institution (school, church, hospital, government, political regime), against decisions made over one’s head, or being forced to do something against one's will. Children suffer the conflict at an early age, when they resist daycare, kindergarten, or school, or when they strongly oppose what they are told to do.
CONFLICT-ACTIVE PHASE: During the conflict-active phase the function of the beta islet cells is reduced, causing hyperglycemia (high blood sugar) or diabetes (compare with alpha islet cells-related diabetes; see also diabetes insipidus related to the kidneys). The biological purpose of storing glucose in the blood is to prepare the individual for the conflict resolution by providing the organism, particularly the muscles, with sufficient amount of blood sugar in order to be able to fight with full force. The degree of hyperglycemia (how much “fuel” will be available) is determined by the intensity of the conflict. For additional support, the liver also secretes glucose, a process called gluconeogenesis. Biologically speaking, the active fight, the response of standing up and to breast, is the distinctive male response to a resistance conflict, whereas the female reaction to a fear-disgust conflict is backing off (fainting).
Typical for diabetes is extreme thirst, which serves the purpose to dilute the high blood sugar level (just as the craving for sweets serves to balance the low glucose level in case of hypoglycemia). What is known as diabetic ketoacidosis is a condition where the liver produces in response to the shortage of insulin high levels of ketone bodies through the breakdown of fatty acids. The function of ketones is to provide energy to the body cells when glucose is in short supply due to the lack of insulin. However, if the levels of ketones are too high, the blood becomes overly acidic, which can lead to serious complications.
With lasting conflict activity diabetes becomes chronic. This is called insulin-dependent diabetes and categorized as type 1 diabetes, also referred to as juvenile diabetes since it apparently occurs predominantly in children and adolescents (compare with type 2 diabetes or adult-onset diabetes). In this case, insulin therapies and dietary measures are vital until the conflict has been resolved.
It is a wide-spread belief that high blood sugar causes damage to the arteries and “indirectly” to the nerves leading to a loss of sensation, especially in the extremities. However, not every diabetic develops the condition! Neither can this theory explain why an elevated glucose level would, for example, affect the feet (or just one foot or toe) in one person and the arm(s) in another. Based on GNM, what is called “diabetic peripheral neuropathy” is a combination of two Biological Special Programs running simultaneously: one involves the beta islet cells of the pancreas linked to a “resistance conflict” causing diabetes, the other involves the periosteum related, in case of the legs, to “wanting to kick somebody away” (usually the person one resists) with the development of leg ulcers or gangrene, depending on the intensity and duration of the conflict (see also “diabetic retinopathy”).
HEALING PHASE: During the first part of the healing phase, in PCL-A, the glucose level decreases to a normal level. However, for the period of the Epileptoid Crisis, when the conflict-active symptoms are reactivated, the blood sugar rises temporarily. Acute hyperglycemia (hyperglycemic shock) can induce a “diabetic coma”! In PCL-B, the blood sugar level decreases below the normal range showing the symptoms of hypoglycemia (compare with alpha islet cells-related hypoglycemia in the conflict-active phase). At the end of the healing phase, the blood sugar level is back to normal. However, with a hanging healing due to continuous conflict relapses, hypoglycemia becomes chronic (and so does the craving for sweets).
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||






{kind=link}