
EARS
 DEVELOPMENT AND FUNCTION OF THE MIDDLE EAR AND EUSTACHIAN TUBES: The ear consists of a peripheral and a central part separated by the eardrum or tympanic membrane. Sound waves captured from the external environment by the outer ear are first transformed by the tympanic membrane into mechanical vibrations, which are transmitted to the ossicles (malleus, incus, stapes) that carry the sound to the inner ear. From there, the acoustic waves pass along the vestibulocochlear nerve to the brain for interpretation. The Eustachian tubes connect the middle ear to the mouth and nasopharynx. They help to keep air pressure in the ears at the right level. In evolutionary terms, the middle ear and Eustachian tubes developed from the intestinal mucosa of the original gullet. Equal to the intestinal cells that absorb (absorptive quality) and digest (secretory quality) the “food morsel”, the biological function of the middle ear and Eustachian tubes is to “insalivate” and “digest” the “sound morsel”. The middle ear and Eustachian tubes consist of intestinal cylinder epithelium, originate from the endoderm and are therefore controlled from the brainstem.
BIOLOGICAL CONFLICT: The biological conflict linked to the middle ear and Eustachian tubes is a “morsel conflict”, specifically, a conflict related to a “sound morsel”.
RIGHT MIDDLE EAR AND RIGHT EUSTACHIAN TUBE
The desired “sound” might concern the voice of a particular person. Newborns and infants suffer the conflict when they can’t “catch” the reassuring voice of the mother. A praise (at school, at home, at work), an acknowledgment, an approval, an offer, a compliment, a proposal, a promise, an apology, a confession, or the “I love you”-morsel one is “drooling” to hear could activate the conflict. In biological terms, the “sound morsel” is equal to nourishment. A hearing conflict can also be experienced when an important message (an announcement) or a sound (telephone ring, baby phone, siren or other acoustic warning signals) were overheard causing a predicament. The much desired “sound morsel” could also be the “sound of silence”.
LEFT MIDDLE EAR AND LEFT EUSTACHIAN TUBE
Such an undesired “sound morsel” relates to any “acoustic dirt” one wants to “evacuate”, for example, an insult, verbal assaults, an accusation, complaints, scolding, criticism, distressing news, hearing something upsetting, the voice of a nagging boss, colleague, parent or spouse or, for a newborn, the voice of a stranger.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase, cells in the middle ear or Eustachian tube proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to be better able to absorb (right ear) or expel (left ear) the “sound morsel”. Hence, during conflict activity the hearing ability is actually enhanced (in Nature, hearing the approach of a predator or other potential dangers is essential for survival). If the conflict persists, a flat (absorptive type) or compact growth (secretory type) develops in the ear. With prolonged conflict activity the cell buildup could completely fill the middle ear or occlude the Eustachian tube. The Eustachian tubes convey air from the back of the nose into the middle ear to equalize ear pressure. Once a Eustachian tube is blocked, the vacuum created in the ear pulls the eardrum inward making hearing difficult as the retracted eardrum can no longer vibrate. As a result, the ear feels blocked.
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. Healing symptoms are ear discharge and earaches due to the swelling with some degree of hearing loss. This is commonly called a middle ear infection (otitis media). When healing takes place in the Eustachian tube, the discharge flowing into the middle ear simulates a “middle ear infection”. Candidiasis in the ear occurs when fungi assist the healing process.
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells remain. Eventually, the growth becomes encapsulated with connective tissue. In conventional medicine, this is usually diagnosed as an ear polyp.
Chronic or recurring ear “infections” indicate that the hearing conflict has not been completely resolved (hanging healing). The constant tissue repair can lead to a perforation of the eardrum with pus continuously draining from the middle ear. Eventually, the hearing ability becomes impaired (compare with hearing loss related to the inner ear). Oftentimes, the distress of “not being able to catch a sound morsel” triggers further hearing conflicts worsening the condition. Hence, learning GNM before symptoms arise is real preventive medicine.
Hearing difficulties generate easily a self-devaluation conflict involving the small bones in the middle ear (malleus, incus, stapes). Over time, the continuing calcification of the ossicles causes otosclerosis, which contributes to the hearing loss.
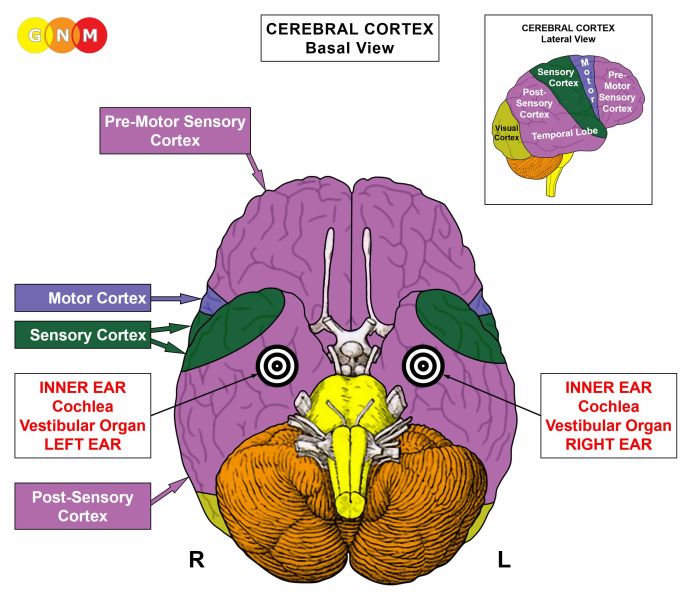
ACOUSTIC NEUROMA: According to conventional medicine, an acoustic neuroma is a “brain tumor” (glioma) on the acoustic nerve (compare with optic neuroma). The “tumor” is also termed “vestibular schwannoma” since the growth consists in addition to neuroglia of so-called “Schwann cells”, a certain type of glial cells. Because of the involvement of the vestibulocochlear nerve, a typical symptom of an acoustic neuroma is in addition to the loss of hearing a loss of sense of balance (see also vertigo related to the inner ear).
In GNM terms, an acoustic neuroma is neuroglia (brain connective tissue) that proliferates during the second part of the healing phase (PCL-B) in order to restore the area of the brain that had received the impact of the hearing conflict.
|






 DEVELOPMENT AND FUNCTION OF THE STAPEDIUS MUSCLE: The middle ear contains three tiny bones or ossicles (malleus, incus, stapes) that carry the sound received from the auditory canal to the inner ear. The stapedius muscle, attached to the stapes, is fundamental in reducing sound transmission. Under normal circumstances, the stapedius is relaxed allowing sounds from the external environment to be perceived with clarity. However, when a sudden intense noise reaches the ear, the muscle contracts in order to dampen the sound to protect the inner ear from damage. The stapedius muscle consists of striated muscles, derives from the new mesoderm and is controlled from the cerebral medulla and the motor cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the stapedius muscle is, according to its function, a noise conflict triggered by unbearable noises such as loud bangs, blasts, explosions, shots, blaring sirens, music with very high decibel levels, a sharp cry, a piercing scream, and the like.
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of stapedius muscle tissue (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing paralysis of the stapedius (controlled from the motor cortex) causing hyperacusis with a decreased sound tolerance, while normal sounds are perceived as very loud (see also hyperacusis with facial paralysis).
HEALING PHASE: During the healing phase, the stapedius muscle is reconstructed. The paralysis (hyperacusis) reaches into PCL-A. The Epileptoid Crisis manifests as stapedial muscle spasms (equivalent to a focal seizure) creating a painful fluttering sensation in the ear. In PCL-B, the function of the stapedius returns to normal.
|

 DEVELOPMENT AND FUNCTION OF THE COCHLEA: The cochlea is a spiral-shaped cavity in the inner ear. It is the actual sensory organ of hearing. The cochlea receives the sound waves from the outer ear and auditory canal and converts them into electrical impulses that are transmitted to the brain via the auditory nerve for interpretation. The auditory nerve, or vestibulocochlear nerve, is divided into the vestibular branch, concerned with balance and motion, and a cochlear division responsible for hearing. The cochlea originates from the ectoderm and is therefore controlled from the cerebral cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the cochlea of the inner ear is a hearing conflict experienced as “I don’t want to hear this!”. Aggravating noises such as dog barking, a screaming child, construction noise (jackhammers, chainsaws, generators), traffic noise (loud trucks, sirens from ambulances, fire engines, or police cars), noisy neighbors, lawn mowers, grass trimmers, loud or annoying music, the nagging voice of a person, or something upsetting that has been said (“I can’t believe what I just heard!”) are examples of what might trigger the conflict. Often, hearing conflicts occur on the phone. Musicians and music lovers with very fine ears can suffer a hearing conflict during a poor musical performance. For someone who is noise-sensitive, the smallest noise can cause ear-related distress.
CONFLICT-ACTIVE PHASE: functional loss of the cochlear branch of the vestibulocochlear nerve resulting in the perception of sounds in one or both ears without an external source. This condition is called tinnitus (compare with hyperacusis caused by a noise conflict, linked to the stapedius muscle).
The ringing, buzzing, humming, whistling, clicking, tinkling, hissing, roaring, and the like, is a frequency of the sound associated with the hearing conflict. The biological purpose of the tinnitus is to be a warning signal saying “last time you heard this, you were in danger. Watch out!”. This explains the variety of sounds heard by people with tinnitus. Depending on the magnitude of the conflict, the sounds or noises can be mild and only noticeable in a quiet room or become extremely loud causing difficulties hearing external sounds (compare with hearing loss in the healing phase). A person might also hear complete sounds or noises such as engine noise, the ringing of a telephone, a musical tune (“music tinnitus”), or a recurring sentence or word (“word tinnitus”). If the tinnitus is present all the time, this indicates that the conflict has not been resolved. Potentially, the tinnitus sound itself causes a hearing conflict, leading to a chronic condition (hanging conflict).
When two hearing conflicts are associated with sounds and noises, the person will develop a double “sound tinnitus” affecting both ears. If, however, one of the two conflicts or both were triggered by the voice(s) of person(s), this leads to hearing voices. In GNM we call this a Hearing Constellation. Conventional medicine considers hearing voices a mental disorder (“paranoid schizophrenia”). In the context of GNM, hearing voices is essentially a double tinnitus with the difference that instead of hearing one or more sounds, a person hears one or more voices. The voice(s) correspond to those that were heard when the original hearing conflicts occurred. Traumatic hearing conflicts can result in severe auditory delusions.
HEALING PHASE: During the healing phase (PCL-A) the volume of the tinnitus sound decreases. However, the swelling created by the edema (fluid accumulation) in the inner ear causes, for the time being, hearing impairment (a loss of the frequencies of the tinnitus sound) or hearing loss in the affected ear (compare with hearing impairment related to the middle ear). Once the edema has been expelled (during the Epileptoid Crisis) the hearing ability slowly returns to normal, provided there are no conflict relapses. Triggers that reactivate a hearing conflict could also be a smell (the odor of the “messenger”) or a visual track (the site of the acoustic source). With a hanging healing, the tissue in the inner ear eventually wears out leading in the long run to deafness. This is why it is important to identify and resolve the original conflict as soon as possible.
Hearing difficulties often trigger self-devaluation conflicts because of “not being able to hear well”. This affects the small bones (malleus, incus, stapes) in the middle ear, which can result in a permanent hearing loss (see otosclerosis). Using a hearing-aid while the inner ear undergoes healing can, therefore, have a highly encouraging effect.
|


 DEVELOPMENT AND FUNCTION OF THE VESTIBULAR ORGAN: The vestibular system is the region of the inner ear where the semicircular canals join with the cochlea. It is the part of the ear that regulates the sensation of balance and motion (the cochlear branch of the vestibulocochlear nerve is responsible for hearing). The vestibular organ originates from the ectoderm and is therefore controlled from the cerebral cortex.
BIOLOGICAL CONFLICT: According to its function, the biological conflict linked to the vestibular organ is a balance conflict, more precisely, a falling conflict. Any fall (accidental fall in sports, at work, falling down the stairs, slipping on a wet or icy surface, a fall from a ladder, tripping over a cable) could trigger the conflict. Certain professions (builders, construction workers, roofers) but also infants and the elderly are more at risk. People with ALS or MS, who have difficulties balancing, often live in fear of falling; the same holds true for epileptics. The conflict also relates to seeing someone else fall or collapse (witnessing someone having a stroke or a heart attack) or hearing that a loved one fell or “dropped dead”. In a transposed sense, the conflict could be experienced as a “fall from grace” or as feeling “dumped”, let’s say, after a separation.
CONFLICT-ACTIVE PHASE: functional loss of the vestibular branch of the vestibulocochlear nerve resulting in a loss of balance, a condition called vertigo (see also acoustic neuroma and vertigo with a “middle ear infection”).
The symptom of vertigo is a sensation of spinning, swaying or falling to one side (vertigo “spins” should not be confused with light-headed dizziness). Whether the tendency is to fall to the right or left is determined by a person’s handedness and whether the conflict is mother/child or partner-related. Hence, if a right-handed person has a mother-related falling conflict, there is a tendency to fall or spin to the left, that is, “towards the mother” (with the Hamer Focus on the right side of the cortex); if the conflict is partner-related, the tendency is to fall or spin to the right, that is, “towards the partner” (with the Hamer Focus on the left side of the cortex). For left-handers, it is reversed. If the conflict concerns oneself, the falling or spinning always tends to the side which relates to the original conflict. For example, if the DHS was a fall to the left, the specific vertigo symptom is also a sensation of spinning or falling to the left.
HEALING PHASE: During the healing phase the dizziness diminishes. The Epileptoid Crisis manifests as a sudden vertigo fit, potentially with severe nausea and vomiting. The extent of the Epi-Crisis is determined by the intensity and duration of the conflict-active phase. Recurring vertigo attacks are triggered by setting on a track that was established when the original falling conflict occurred. Alcohol, for example, could be such a track.
If the falling conflicts affect the vestibular organ of both ears this causes, in GNM terms, a Vertigo Constellation. The symptoms are a wide-based and unsteady stance and gait with reeling or lurching movements. The medical term for this condition is ataxia or Friedreich’s ataxia. The physical incoordination and clumsiness is not the result of muscle weakness but due to the unbalanced equilibrium caused by the “double vertigo”. Since infants and the elderly are more likely to suffer falling conflicts, ataxia develops more often in childhood and in later life.
Meniere’s disease, also known as primary endolymphatic hydrops, is, according to conventional medicine, “an inner ear disorder that affects balance and hearing”. Based on GNM, the condition is a conflict combination of a falling conflict (involving the vestibular organ) and a hearing conflict (involving the cochlea).
|
 DEVELOPMENT AND FUNCTION OF THE OUTER EAR AND AUDITORY CANAL: The auditory canal extends from the outer ear to the eardrum (tympanic membrane). The outer ear, or auricle, is made up of cartilage covered with skin (corium skin and epidermis). The main function of the outer ear is to capture sound from the external environment and carry it through the auditory canal to the middle ear, where the acoustic wave is transformed into vibrations reaching the inner ear. The lining of the outer ear and of the ear canal consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the outer ear and auditory canal is a “separation conflict” associated with the ear. The conflict is experienced as a loss of skin contact at the outer ear, including the earlobe, or as not wanting to be touched at the ear or in the ear (licking or kissing the ear, unpleasant ear examination procedures, manipulation in the ear canal). Wanting to get rid of something in the ear, for example of water, could also trigger the conflict.
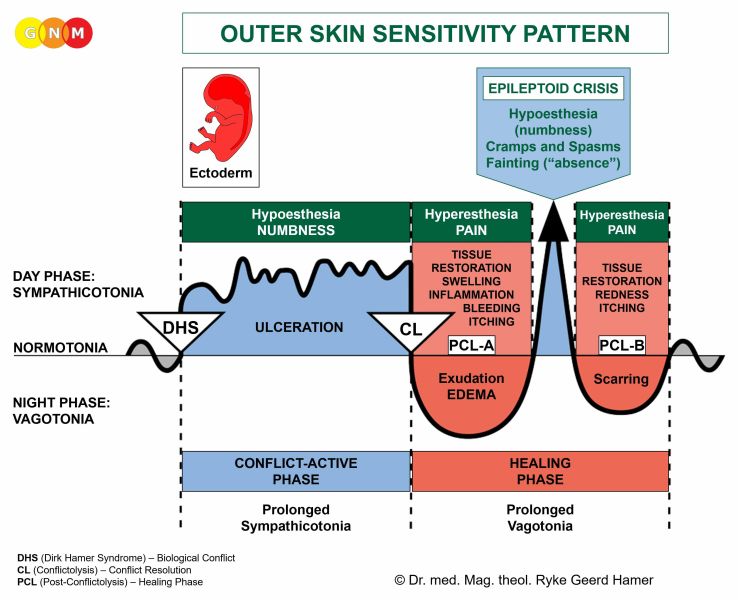
CONFLICT-ACTIVE PHASE: ulceration in the epithelial lining of the outer ear and/or the ear canal. With intense or prolonged conflict activity, the ulceration makes the skin dry and flaky; with acute conflict activity the skin on or in the ear feels numb (see Outer Skin Sensitivity Pattern above).
HEALING PHASE: During the healing phase the ulcerated area is replenished with new cells. Typical healing symptoms are itchy ears and, if the healing process is more intense, a skin rash with inflammation and redness. The healing process in the ear canal might be accompanied by clear discharge, commonly called “swimmer’s ear”. A large swelling, termed a cholesteatoma, can cause a blockage in the auditory canal resulting in hearing difficulties until the healing process is complete.
|

 DEVELOPMENT AND FUNCTION OF THE EAR CARTILAGE: The ear cartilage forms the shape of the ear and the outer third of the auditory canal. It consists of elastic connective tissue covered by a thin layer, called the perichondrium (unlike other connective tissue, cartilage does not contain blood vessels). The ear cartilage originates from the new mesoderm and is therefore controlled from the cerebral medulla.
BIOLOGICAL CONFLICT: The biological conflict linked to the ear cartilage is a self-devaluation conflict associated with the ear (compare with self-devaluation conflict related to the ossicles). Generally, the conflict is experienced as “my ears are worthless”, let’s say, because of having missed an important message. Being hard of hearing and therefore not being able to follow a conversation might also cause the conflict.
CONFLICT-ACTIVE PHASE: necrosis (cell loss) of cartilage tissue, which goes unnoticed.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation with swelling due to the edema (fluid accumulation). If bacteria are available, they will assist the healing process. With an inflammation, the condition is called perichondritis.
| |||||||||||||||||||





{kind=link}