
SKIN
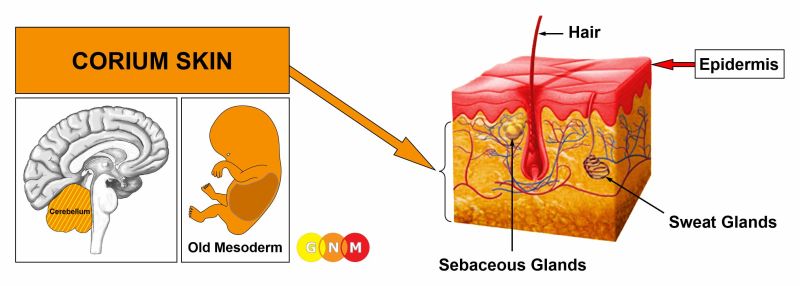
DEVELOPMENT AND FUNCTION OF THE CORIUM SKIN: The skin consists of two main layers, namely, the epidermis (outer skin) and the corium skin (dermis or under skin). The function of the relatively thick dermis is to protect the organism against injury and attacks. The corium skin is composed largely of melanocytes, which are the cells that make the pigment melanin that gives color to the skin and hair (melanin is also produced in the iris and ciliary body of the eyes). Melanin acts as an effective absorber of light to shield the skin from UV radiation. Embedded in the dermis are sebaceous glands and sweat glands. In evolutionary terms, the corium skin developed together with the pleura, the peritoneum, and the pericardium. The corium skin, including the sebaceous glands and sweat glands, originates from the old mesoderm and is therefore controlled from the cerebellum.
NOTE: The clitoris and glans penis are covered by an epidermal skin layer but not endowed with a corium skin. With the rise of mammals, the breast glands developed from the sweat glands in the corium skin.
|
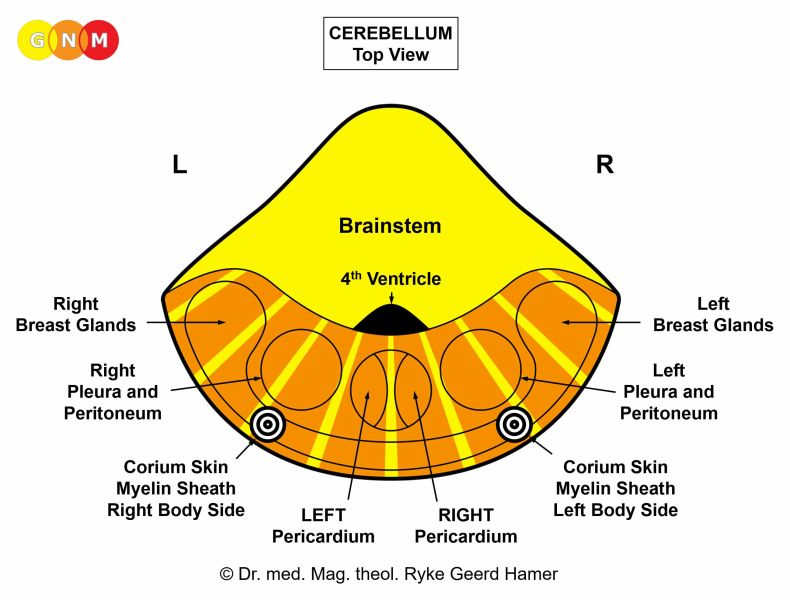 | BRAIN LEVEL: In the cerebellum, the corium skin (including the sebaceous glands and sweat glands) of the right half of the body is controlled from the left side of the brain; the corium skin of the left half of the body is controlled from the right brain hemisphere. Hence, there is a cross-over correlation from the brain to the organ.
NOTE: The myelin sheath is controlled from the same brain relay as the corium skin (see also eyelid glands).
|
BIOLOGICAL CONFLICT: According to its protective function, the biological conflict linked to the corium skin is an attack conflict (see also attack conflicts related to the pleura, peritoneum, and pericardium).
In line with evolutionary reasoning, attack conflicts are the primary conflict theme associated with cerebellum-controlled organs deriving from the old mesoderm.
|
An attack conflict is experienced, for instance, through an attack by a person or by an animal or through a hit or blow against the body or against the head (in sports, in a fight, in an accident). However, medical procedures such as surgery (the image of being cut with a scalpel), a needle biopsy, injections, vaccinations as well as stabbing or piercing pain could also be registered as an “attack”. Verbal attacks, for example, being yelled at, scolded, assaulted or threatened with sharp and aggressive words typically “hit” the face, the forehead (an insult against one’s intelligence), or the back (“stab in the back”). Sexist remarks, sexual accusations, or an attack against one’s sexual orientation usually strike “below the waist”. Hearing offensive words affects the corium skin of the ear. Being criticized in a hostile manner, discrimination, defamation, or an insult against one’s integrity could have an impact on the whole body (generalized conflict). A skin condition such as acne or surgical scars in the face or on the body (after a mastectomy) can evoke a disfigurement conflict which also corresponds biologically to the corium skin.
In addition, the conflict linked to the corium skin relates to feeling unclean (smelly sweat, stinky feet, malodorous discharge, incontinence) or feeling soiled, for example, when coming in contact with something considered as repellent such as dirt, feces, urine, vomit, saliva, (menstrual) blood, sweat, or semen. “Dirty” words thrown at one’s face or gossiping behind one’s back might provoke the conflict, because the psyche, in GNM terms, cannot differentiate between real dirt and figurative dirt. A “feeling soiled” conflict could be triggered through physical contact with a person who is regarded as “repulsive”, for instance, a drunk person, a smelly person, or a person who has a “contagious disease” (venereal disease), provided that one believes that “infectious diseases” are transmittable. The fear of an “infection” and of contracting a disease can affect an entire population (see epidemics such as the Great Plague).
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase melanocytes in the corium skin proliferate at the “attacked” or “soiled” site forming a compact growth or melanoma. In conventional medicine, the growth is considered a skin cancer (see also basal cell cancer and squamous cell skin cancer). From an evolutionary viewpoint, however, a melanoma is an archaic form of defense that serves the biological purpose to provide a protective layer or “thicker skin” against further attacks (see also pleural mesothelioma, peritoneal mesothelioma, pericardial mesothelioma). – Occasionally, melanin deposits occur in atypical locations. In the presence of a “primary skin cancer”, the accumulation of melanin, presenting as brown pigments, for example in the liver or in the brain, is erroneously diagnosed as a “metastatic melanoma” (see GNM Article “Questioning the Metastasis Theory”).
NOTE: Excessive UV radiation from the sun can certainly damage the skin but does not cause skin cancer, as claimed. It is rather the fear of skin cancer that results in the development of a melanoma. Sun lotions don’t protect the skin from “cancer” but reduce the fear of getting skin cancer! Besides, melanomas and other types of skin cancer appear on areas of the body that have not been exposed to the sun. Neither does the UV-theory explain why a skin cancer occurs on a very specific location (on the cheek, on the breast, on the back), why on the right or left side of the body, and why at a certain time in a person’s life.
|
 | If the melanoma is pigmented it appears as black, brown or blue. A melanotic melanoma always involves a mole. Moles are remnants of the dark-pigmented skin that once covered the entire body as a protection against excessive sun exposure, which is still seen in dark-skinned people living at lower latitudes such as in tropical Africa. Light skin pigmentation as found in the European population evolved much later.
|
 | A non-pigmented or amelanotic melanoma appears as pink since it does not contain pigments (see shingles).
|
NOTE: Whether the right or left side of the body is affected is determined by a person’s handedness and whether the conflict is mother/child or partner-related. A localized conflict affects the area of the skin that is associated with the attack or with “feeling soiled”.
|
The appearance of a melanoma can provoke a disfigurement conflict with the result that in a short period of time other melanomas occur in the same area. A surgical removal of the growth might trigger an attack conflict leading to the development of new melanomas – a vicious cycle for someone who is not familiar with GNM.
 | What is termed Kaposi sarcoma (KS) are “tumors” that show as purple or brown blotches. They present the typical picture of melanomas. Yet, in conventional medicine, the growths are nowadays considered an AIDS-defining illness (see also shingles): “AIDS-related Kaposi sarcoma arises in people who are infected with HIV. It was in part the unusual and sudden appearance of this form of KS in so many young men at the start of the AIDS epidemic that led doctors to realize that a new disease had emerged” (Is Homosexuality a Health Risk?). Based on the knowledge of GNM, the rise of “the new disease” was caused by the fear associated with HIV and AIDS (“feeling soiled” or “infected” by a person who is “HIV positive” or feeling attacked because of one’s sexual orientation) rather than by a virus that has never been proven to exist.
|
HEALING PHASE: Following the conflict resolution (CL), fungi and TB bacteria or other bacteria remove the cells that are no longer needed. The involvement of TB bacteria causes skin tuberculosis.
 | During the decomposing process, the melanoma changes its texture (the growth becomes soft and spongy), its shape (it becomes larger and asymmetric with uneven edges), and it might bleed. When the overlying epidermis opens, the smelly discharge produced by the TB bacteria breaks through the skin (see also healing phase of glandular breast cancer).
|
If the required microbes are not available at the time, the growth remains. However, with constant conflict relapses the melanoma continues to grow.
A carbuncle or furuncle, also known as a boil or skin abscess, is a nodule filled with pus produced by the bacterial activity in the corium skin. Carbunculosis or furunculosis occurs with recurring conflict relapses. A furuncle or carbuncle could also originate in the connective tissue; in this case, the related conflict is a self-devaluation conflict. A pilonidal cyst is a boil that develops on the tailbone near the cleft of the buttocks as the area where the attack conflict was registered. Interestingly, the condition was widespread in the United States Army during the Second World War. It was termed “jeep riders’ disease” because a large number of soldiers who were being hospitalized for it rode in Jeeps. The prolonged rides in the bumpy vehicles must have triggered an “attack” conflict.
 | This picture shows several boils spread over both sides of the upper back. Malicious badmouthing behind one’s back would be a conflict scenario of an attack conflict perceived at this particular area of the body.
|
THE GREAT PLAGUE (1348-1351)
The Great Plague is estimated to have killed 30-60% of Europe’s total population. It is said that the disease was brought to Europe through trade ships carrying infected rats. Curiously, the rats did not get the plague!
| |
 | Symptoms of the bubonic lpague: dark, purple swellings with the characteristic foul-smelling discharge indicating a skin tuberculosis, linked to a “feeling soiled” conflict and the panic of contracting an “infectious disease” (the plague).
Symptoms of the pneumonic plague: a cough with bloody sputum and hemorrhaging of the lungs indicating a lung tuberculosis, linked to a death-fright conflict (fear of the “deadly plague”). NOTE: 95% of the people died of the pneumonic plague!
|
In 1894, the Swiss physician Alexandre Yersin, a student of Louis Pasteur, examined plague victims in Hong Kong. Under the microscope he found masses of bacteria. He asserted that these bacteria had caused the Great Plague and named the bacterium Yersinia pestis. One of Yersin’s students claimed that he had found the Yersinia pestis bacillus in the stomach of rat fleas. He argued that the flea bite had injected the people with the bacteria…
In March 2014, after the excavation of a mass grave in London with plague victims of the 14th century, researchers analyzed the teeth of some of the skeletons. The teeth contained indeed the DNA from the bacterium Yersinia pestis (termed “Yersinia pseudotuberculosis”!). However, the DNA analysis revealed that “the Black Death was not bubonic plague, as has been thought, but pneumonic plague” (Health and Medicine, March 31, 2014). This confirms that the Great Plague was, in reality, an epidemic of death-fright conflicts (triggered by the “deadly disease”) that had seized the European population.
| |
 | In leprosy (linked to attack conflicts) the growths develop on a flat plane rather than forming compact boils. However, like open pest-boils (see bubonic plague) the tubercular discharge (skin tuberculosis) produced by the Mycobacterium leprae has a foul-smelling odor. The continuous repair processes (hanging healing) in the dermis lead eventually to disfiguring skin sores, usually due to the condition itself (feeling soiled and disfigured).
|
Smallpox is allegedly caused by the so-called variola major virus. It is speculated that the virus evolved from a rodent virus between 68,000 and 16,000 years ago. Starting in 1967, the World Health Organization ordered a global vaccination program against smallpox; the “disease” was supposedly eradicated in 1979.
 | Smallpox presents as sharply raised pustules.
In the 1600s European “settlers” first brought smallpox to North America. In 1633-1634 the disease (in reality “attack conflicts”) wiped out entire Native American tribes. NOTE: Death of smallpox usually occurred from pneumonia, generated by territorial fear and existence conflicts!
|
 | This image shows the clinical picture of pustular eczema. The pus-filled papules on the skin appear on an inflamed surface (see dermatitis). In this case, the Biological Special Programs of the corium skin (attack or “feeling soiled” conflict) and of the epidermis (separation conflict) run concurrently.
|
Shingles are small, non-pigmented (amelanotic) growths that develop along one or several segments of the skin. During the healing phase, the skin lesions become swollen and red due to the inflammation and the blisters are filled with pus produced by the bacteria. After the Epileptoid Crisis, in PCL-B, the blisters dry up, form scabs, and gradually fade away. The scarification process is accompanied by acute sharp, stinging pain. This is characteristic for the healing of all old-mesodermal tissues (see also glandular breast cancer). Recurrent bouts of shingles are triggered by conflict relapses through setting on a track that was established when the original attack or “feeling soiled” conflict took place.
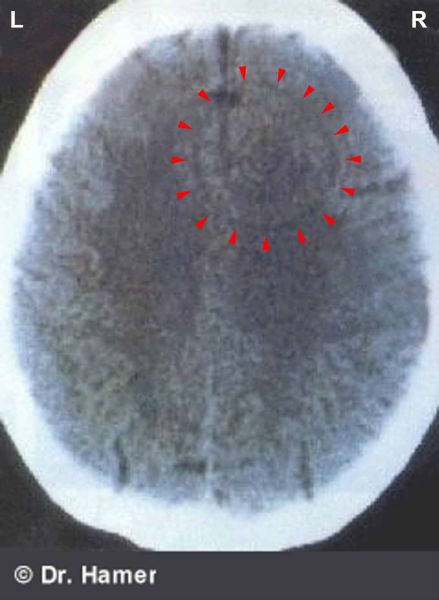
Conventional medicine claims that shingles are caused by a reactivation of a previous infection with the “varicella-zoster virus”, a type of “herpes virus” that supposedly causes chickenpox (by the same token it is said that people who had chickenpox have a “lifelong immunity” against a new “infection” with the “zoster virus”). It has been suggested that the virus migrates along the sensory peripheral nerves, replicates at the area of the skin supplied by that nerve, which then results in the development of shingles. The virus theory, however, cannot explain why the “virus” would affect a very specific skin segment (face, shoulder, thorax, torso, genital area) and why the condition occurs on the right or left side of the body or on both. The immune system theory does not provide any answers either. Besides the fact that the existence of the alleged virus is highly questionable, Dr. Hamer's research demonstrates that every person with shingles shows on the brain scan the Hamer Focus in the cerebellum, precisely, in the area of the brain that controls the corium skin (see brain scan below); hence, the activity of bacteria(!) in the healing phase. The skin rash that occurs with chickenpox, on the other hand, involves the epidermis and is controlled from the cerebral cortex.
 | On this brain scan, the orange arrow points to a small edema on the right side of the cerebellum (view the GNM diagram). It is an indication that an attack or “feeling soiled” conflict has been resolved. In the healing phase, shingles developed on the left side of the body.
|
 | Shingles on the left torso reveal that the conflict (feeling attacked or soiled “below the waist”) was associated with a partner, if the person is left-handed. For right-handers, the conflict would be mother/child-related.
NOTE: The shingle rash can involve simultaneously the corium skin (feeling soiled) and the epidermis (e.g., wanting to separate from a repulsive person; see herpes).
|
Like Kaposi sarcoma, in conventional medicine shingles is construed as a “disease” related to AIDS: “In the days before the HIV/AIDS pandemic, shingles used to be seen only in older people or in those who had weakened immune systems. Nowadays shingles are very common with HIV infections and AIDS” (health24, January 10, 2012).
Candidiasis of the skin (subcutaneous candidiasis) occurs when fungi assist healing. In the genital area, this might be provoked by “unclean” sex, “dirty” sexual practices, or feeling “soiled” through sexual insults (compare with vaginal candidiasis and penile candidiasis). In sick or elderly people requiring nursing care “dirty diapers” typically cause candidiasis in the genital and anal region.
A fungal infection of the skin is also commonly known as “ringworm”. The medical term for ringworm is tinea. It has nothing to do with a worm.
 | Tinea versicolor is a skin condition that presents as hyperpigmentation (in the conflict-active phase) or hypopigmentation (in the healing phase). The white patches are the result of lasting fungal activity, or hanging healing, leading to the depigmentation of the corium skin (compare with white skin patches in vitiligo related to the epidermis).
|
 | A nail fungus (tinea unguinum or onychomycosis) develops in the corium skin underneath the nail plate of the toe or fingernails through coming in contact with something considered as “disgusting” (see also Athlete’s Foot).
|
The sebaceous glands are exocrine glands that secrete an oily substance (sebum) to lubricate the skin. They are most abundant in the face and scalp. The distress over getting bald (a typical male concern) or over a hairdo (a typical female concern) could therefore be the underlying cause for having a greasy scalp.
Acne is, in GNM terms, linked to an attack or “feeling soiled” conflict. The inflammation with swelling, redness, and pustules filled with pus is already the healing phase, assisted by bacteria (Propionibacterium acnes). During the conflict-active phase, the skin appears bumpy. Depending on the intensity of the conflict, the condition ranges from small pimples to a severe skin condition. The theory that acne is related to hormonal changes is inconclusive, because not every teenager has acne and adults have it too.
 | Acne most commonly appears on the face, particularly in puberty since adolescents are much more vulnerable concerning their looks. Feeling unattractive or not good looking can therefore easily lead to acne. Also, the teenage years are the time where there are more confrontations (verbal attacks) with adults (parents, teachers, authorities). Usually, it is the appearance of acne itself (feeling “soiled” in the face) that delays the completion of the healing process.
|
 | A sebaceous cyst (epidermoid cyst) is a lump beneath the surface of the skin filled with yellowish sebum (see also stye and chalazion related to the sebaceous glands in the eyelids; compare with fat nodules, or xanthomas).
A sebaceous cyst on the forehead reveals an attack conflict related to an intellectual performance (“You fool!”). For a left-hander, a cyst on the left side points to a conflict associated with a partner.
|
 | Trichilemmal cysts, also known as wen, originate in a hair follicle in the dermis. They are therefore often found on the scalp, which has a high hair follicle concentration. The cheese-like odor of the cysts is a sign that mycobacteria are at work.
|
The sweat glands in the corium skin produce a watery, salty film that regulates the body temperature and prevents the organism from drying out. Moreover, the sweat glands are responsible for the elimination of metabolic waste (see also night sweats). Sweating is regulated by the sympathetic nervous system, which is why perspiration increases with stress, nervousness, or excitement and during conflict activity (cold sweats).
In the conflict-active phase of an attack or “feeling soiled” conflict the sweat gland cells proliferate causing excessive sweating (hyperhidrosis). Depending on the individual conflict situation, the sweating can either be generalized or confined to a specific area of the body such as the armpits, groin, palms of the hand, soles of the feet, or the scalp (localized conflict). In the course of the healing phase, the additional sweat gland cells are removed by fungi or bacteria accompanied by a strong body odor (compare with body odor caused by night sweats).
Tinea pedis is a “fungal infection” involving the sweat glands in the feet (compare with nail fungus). The “feeling soiled” conflict typically occurs when the feet come in contact with something “dirty”, for example, through walking on filthy floors (public showers, locker rooms, washrooms), wading in dirty water, or stepping on animal poop. Sweaty boots, sweaty shoes, or sweaty socks considered as “yucky” also trigger the conflict. During the healing phase, the fungi produce a cheese-like substance that creates the distinctive smell of “Athlete’s foot” (the term became popular since the condition is common among athletes). The smelly feet usually lead to new “feeling soiled” conflicts with the consequence that the fungal activity continues. Shoes associated with the smelly feet or dirty public facilities can become a track leading to a chronic condition. The reason why remedies such as “walking barefoot on morning dew grass” work is that the feet are no longer associated with being “soiled” but instead with being fresh and clean, which clears the tracks allowing the completion of the healing phase.
NOTE: Whether the attack or “feeling soiled” conflict affects the sebaceous glands or the sweat glands is random. However, the attack conflict related to the corium skin is always experienced as more severe.
|
CORIUM SKIN - SWEAT GLANDS
|
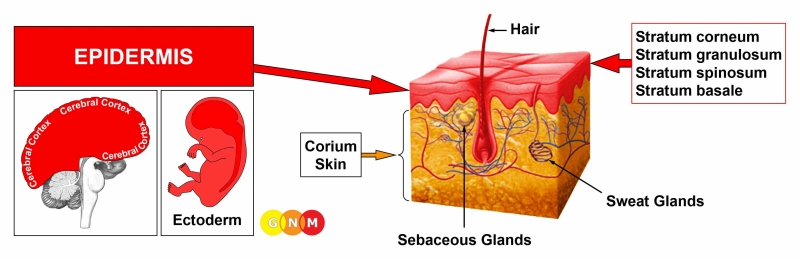
DEVELOPMENT AND FUNCTION OF THE EPIDERMIS: The epidermis (outer skin) covers the underlying corium skin (dermis or under skin). The epidermis is predominantly responsible for sensory perception such as temperature, pressure, and touch. Most cells in the epidermis are keratinocytes (keratin-producing cells) that originate in the deepest layer of the epidermis, called the stratum basale. This layer also contains pigment-producing melanocytes (the majority of melanocytes are, however, in the corium skin). From the basal layer, keratinocytes migrate through the stratum spinosum and stratum granulosum up to the stratum corneum. Once they reach the surface of the skin, they are gradually shed and replaced by newer cells pushed up from below. Keratin is also the main structural component of hair and nails. The epidermis consists of keratinized squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
 | BRAIN LEVEL: The epidermis is controlled from the sensory cortex (part of the cerebral cortex). The skin of the right side of the body is controlled from the left side of the sensory cortex; the skin of the left side of the body is controlled from the right cortical hemisphere. Hence, there is a cross-over correlation from the brain to the organ (see GNM diagram showing the sensory homunculus).
|
BIOLOGICAL CONFLICT: The biological conflict linked to the epidermis is a separation conflict experienced as a loss of physical contact (see also separation conflict related to the periosteum).
In line with evolutionary reasoning, territorial conflicts, sexual conflicts, and separation conflicts are the primary conflict themes associated with organs of ectodermal origin, controlled from the sensory, pre-motor sensory and post-sensory cortex.
|
Newborns suffer the conflict when they are separated from the mother at birth (put in an incubator, given up for adoption). A separation conflict can already occur intrauterine, for example, because of ultrasound procedures. The ultrasound noise drowns out the heartbeat of the mother, which can be highly traumatic for the fetus; each ultrasound test triggers a conflict relapse for the unborn (see Down syndrome). For an infant the mother is the most important attachment figure; the mother protects her child and can prevent conflicts from happening. Hence, when a small child has a separation conflict (or, for example, a scare-fright conflict/territorial fear conflict) then the mother was usually absent when the DHS occurred. Children also experience separation conflicts when they are scolded, punished or abused, when a new sibling is born who gets more attention, when the parents split up, when they are not allowed to see their friends, when they have to separate from a favorite doll, teddy bear, stuffed animal or pet they like to cuddle; also, when the mother goes back to work, when they are put into daycare, kindergarten or to relatives, or when they are left with a sitter or nanny. Similarly, the elderly feel separated from the “pack” when they have to move into a nursing home or after the death of a life-long spouse or companion. The fear of losing touch or contact with someone (the threat of a divorce, a difficult long-distance or weekend relationship, the fear that a loved one might leave, move away, or die) or feeling rejected by a person, let’s say, because of a disagreement can evoke the conflict. Pets suffer separation conflicts, for example, when their master leaves or dies or when they are put in a kennel. By the same token, the conflict refers to wanting to separate from a person in the sense of wanting but not being able to push someone away (literally or figuratively), for example, a terrorizing boss or teacher, an annoying colleague or schoolmate, or an abusive parent or spouse (compare with touch conflict of not wanting to be touched related to the myelin sheath).
A separation conflict also pertains to wanting to separate from something close to the skin (face mask, oxygen mask, a helmet, hat, clothing, shoes, tight stockings, wet linen, wet diapers). The same applies to a separation from something that one is no longer allowed or able to touch (a musical instrument, keyboard, tennis racket, golf club, steering wheel) or feel on the skin (an engagement ring, a favorite pillow) – see localized separation conflict. NOTE: A separation from a home is not a separation conflict in biological terms, since it does not relate to the skin but concerns the “territory” (see territorial loss conflict).
 |
|
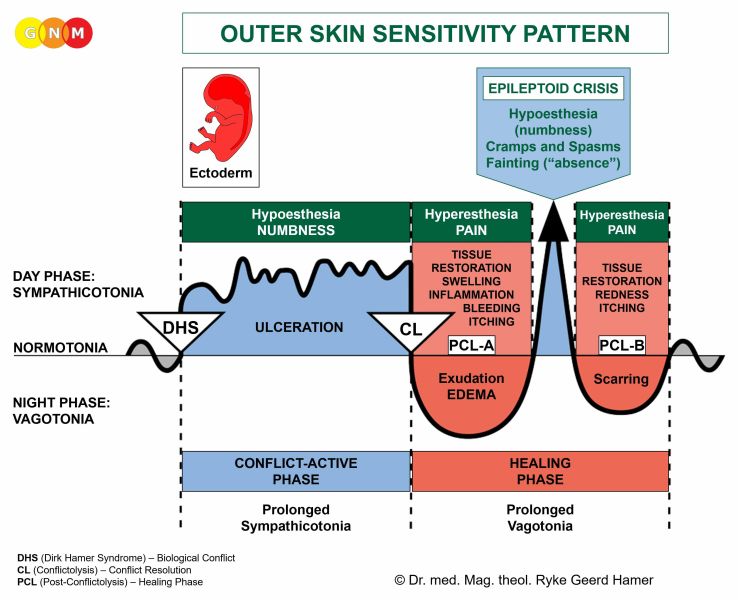
CONFLICT-ACTIVE PHASE: During the conflict-active phase the epidermis ulcerates at the area(s) associated with the separation. The ulcerations are microscopic and usually go unnoticed. With continuing conflict activity, however, the skin becomes dry, rough, flaky, pale, and cold from poor blood circulation. Eventually, the skin begins to crack causing fissures that may bleed (see angular cheilitis; compare with oral conflict related to the mouth surface mucosa). If an intense conflict persists for a long period of time, the skin opens at the ulcerated area (see leg ulcers). Ichthyosis, a skin condition characterized by fine scaling similar to fish-scales, is also an indication of long and intense conflict activity. A severe form of ichthyosis is termed Netherton syndrome, assumed to be a “genetic disease”.
On the scalp, the flaky skin shows as dandruff. Deep ulceration of the epidermal skin causes hair loss (alopecia), also in pets.
 | In this example, the bald spots are exclusively on the left side of the scalp. This reveals that the loss of physical contact (say, missing to be stroked on the head) is related to a partner if the man is left-handed or to his mother if he is right-handed.
With the resolution of the conflict, the hair starts growing back.
|
Because of the loss of epidermal cells the sensitivity of the skin decreases (compare with hyposensitivity related to the periosteum). If the separation conflict is severe the skin can become completely numb (sensory paralysis). Sudden sensory numbness, for example of an arm or leg, is often confused with a stroke. A brief reactivation of the sensory paralysis arises during the Epileptoid Crisis.
A typical symptom of the conflict-active phase is a short-term memory loss, which serves the purpose to temporarily “forget” the one who was “torn from the skin” by blocking out the memory (in the animal world, a mother cat does no longer recognize her offspring when they are separated from her too early). The short-term memory loss reaches into the first part of the healing phase (PCL-A). In children, the poor memory shows as learning difficulties and focusing problems labeled, nowadays, as Attention Deficit Disorder (ADD). In adults, long-lasting separation conflicts can lead to dementia (see also (Post)Sensory Cortex Constellation).
NOTE: Short-term memory loss occurs during any Biological Special Program (in the conflict-active phase and PCL-A) involving the sensory, post-sensory, or pre-motor sensory cortex because, in biological terms, the squamous epithelium of the entire organism is associated with a “separation conflict” (see, for example, biological conflict related to the milk ducts, mouth surface mucosa, nasal mucosa, or upper two-thirds of the esophagus).
|
VITILIGO develops when the ulceration reaches into the basal layer of the skin that consists of melanin-producing cells. The depigmentation creates the white patches typical for vitiligo (compare with tinea versicolor involving the corium skin; see also scarlet fever). The separation conflict related to the deepest layer of the epidermis is – subjectively – perceived as particularly cruel or “brutal” (loss of a loved one, physical abuse). The white macules appear at the site(s) associated with the separation. Hair that grows on areas affected with vitiligo turns white. Albinism, characterized by white skin and white hair, is caused by a generalized, “brutal” separation conflict suffered by the unborn child. Due to the complete loss of the pigmented skin layer a repigmentation is no longer possible, even if the conflict is resolved.
 | Vitiligo on the right side of the trunk reveals a “brutal” separation from a partner (for a right-handed person).
|
During the first part of the healing phase (in PCL-A) the affected area of the skin becomes pinkish and red, followed by a slow(!) repigmentation process in PCL-B. However, recurring conflict relapses during this phase lead to hyper-pigmentation presenting as brown spots, known as café-au-lait spots.
 | Here, the café-au-lait spots are on the left side of the upper body, respecting the midline. Hence, the separation conflict is associated with the mother (for a right-handed person) or with a partner (for a left-handed person).
In conventional medicine, six or more café-au-lait spots are diagnosed as “von Recklinghausen's disease”. According to Dr. Hamer's research, “von Recklinghausen's” relates biologically to the myelin sheath and is linked to a touch conflict (see neurofibroma).
|
 | This picture shows café-au-lait spots (light brown) on the glans penis caused by a severe separation conflict (e.g., not wanting to have sexual contact). The melanomas (dark brown) on the penis shaft correlate to “feeling soiled” (the development of melanomas is confined to the penis shaft since the penis head is not endowed with a corium skin).
|
HEALING PHASE: During the first part of the healing phase (PCL-A) the ulcerated area of the skin is replenished through cell proliferation. The skin swells up, becomes red, inflamed, irritated, itchy, and sensitive to touch (hypersensitivity). The small fluid-filled edemas appear as blisters. After the Epileptoid Crisis, in PCL-B, the blisters dry up and the skin normalizes, provided there are no conflict relapses.
NOTE: All Epileptoid Crises that are controlled from the sensory, post-sensory, or pre-motor sensory cortex are accompanied by troubled circulation, dizzy spells, short disturbances of consciousness or a complete loss of consciousness (fainting or “absence”), depending on the intensity of the conflict. Another distinctive symptom is a drop of blood sugar caused by the excessive use of glucose by the brain cells (compare with hypoglycemia related to the islet cells of the pancreas).
|
 | Under a microscope the ulceration that occurs in the conflict-active phase (left picture) and the small edemas developing in the healing phase (right picture) show as a ring-configuration, strikingly similar to a Hamer Focus (click to view the image) in the correlating brain relay.
|
The healing of the skin manifests as a SKIN RASH, termed dermatitis, eczema, hives (urticaria), measles, rubella, chickenpox, rosacea, lupus, psoriasis, herpes, et cetera. Based on GNM, it is all the same, namely the healing phase of a separation conflict.
SKIN RASH LOCATION
An unwanted separation (not being able or allowed to embrace or hold a beloved person or a pet) typically presents as a skin rash on the inside of the arms, hands, fingers, or legs, while wanting to separate from a person affects predominantly the outside of the arms, hands, elbows, legs, knees, shinbones, or ankles used, figuratively, to push or kick someone away. Depending on the exact conflict situation, focal skin rashes also appear on the head (scalp), face (see also outer skin of the eyelid), lips (cold sores), chest, belly, external genitals, toes and feet (wanting or not wanting to leave a certain place), or on the back. A widespread skin rash (exanthema) reveals a generalized separation conflict suffered by a person as a whole. A body rash can also be caused by poisoning, for example, from medication – without a DHS.
NOTE: Whether the right or left side of the body is affected is determined by a person’s handedness and whether the conflict is mother/child or partner-related. A localized separation conflict affects the area of the skin that is associated with the separation.
|
A chronic skin rash occurs due to persistent conflict relapses through setting on a track that was established when the separation conflict first took place. Thus, with a hanging healing, the skin condition remains until all tracks are cleared. The SYNDROME (a concurrent, active abandonment or existence conflict) worsens the rash. During extended periods of conflict activity, the skin rash disappears (see conflict-active phase). The Biological Special Program is, however, not completed!
NOTE: Topical corticosteroids (see cortisone) used in inflammatory skin conditions interrupt the healing phase. This is why the rash reoccurs shortly after the application is discontinued.
|
Recurring skin rashes are also triggered by the encounter with a conflict track (see allergies). If the rash is on the hands or fingers it is called a “contact eczema” or “allergic contact dermatitis”. Tracks that prompt the flare-up of such eczemas are, for instance, a specific fruit or vegetable, a piece of jewelry (ring or necklace), a certain body care product or perfume, or animal hair (a pet). What is known as dyshidrosis or dyshidrotic eczema is a skin condition in which small, fluid-filled blisters develop on the palms of the hand, on the edges of the fingers or toes, or on the soles of the feet. A so-called heat rash, or “polymorphous light eruption”, is caused by a sun-track associated with a separation conflict (see also “solar herpes”; compare with the development of a “melanoma” related to excessive sun exposure).
 | Babies develop dermatitis around the mouth and on the cheeks when the mother stops breastfeeding too abruptly. The separation conflict is brought on by the loss of contact with the mother’s breast. If the first taste of commercial milk is established as a track, this causes a so-called “milk allergy”.
|
 |
 | Erysipelas is a skin condition characterized by a painful rash (red, swollen, inflamed) with a sharply demarcated border. The affected skin looks very similar to cellulites (see fat tissue) linked to a self-devaluation conflict. This is why it is often difficult to tell apart. The two Biological Special Programs might also overlap due to a self-devaluation conflict caused by the skin condition itself. Sudden symptoms of high temperature, shivering, and vomiting occur during the Epileptoid Crisis.
It is thought that erysipelas develops when bacteria enter the skin through cuts or sores or due to an “immune deficiency”. Based on GNM, the real cause is a separation conflict. The affected area, for example, the right leg (see picture) reveals with what part of the body the separation was associated. Taking into account a person's handedness, the conflict is mother/child or partner-related. We also have to consider a localized separation conflict.
|
 | Both rosacea (left picture) and lupus erythematosus (right picture) are skin rashes that appear on the nose, chin, and cheeks. The conflict is experienced as a separation “from the face” either through a loss of contact or through wanting to separate (“get out of my face!”). The pus-filled pimples (here with rosacea) involve the corium skin and are linked to a disfigurement conflict, usually caused by the skin condition itself.
|
Since the face is supplied by the trigeminal nerve, healing of the facial skin is often accompanied by nerve pain, called trigeminal neuralgia (see also trigeminal neuralgia related to the periosteum and to the facial bones).
 | This CT scan highlights a Hamer Focus in the brain relay that controls the right trigeminal nerve. In this case, the person (a left-handed male) suffered a separation conflict from his mother. The trigeminal neuralgia occurs therefore on the right side of the face.
|
LYME DISEASE
Lyme disease is said to be transmitted to humans by the bite of ticks infected with the bacterium Borrelia burgdorferi. According to the theory, if left untreated the “infection” spreads to other parts of the body.
| |
 | The typical symptoms of borreliosis include fever, body aches, fatigue, headaches, and a circular outwardly expanding rash, called erythema migrans (EM), at the site of the bite. Based on GNM, the characteristic reddening is not the result of an “infection” but rather the healing of the injury caused by the tick bite (the release of histamine enlarges the pores in the blood vessel wall to increase the blood flow at the affected area). The same response occurs, for example, after a bee sting.
|
Symptoms associated with borreliosis such as muscle paralysis, a fungal infection known as “ringworm”, swollen joints, muscle pain, meningitis are brought on by the panic triggered by the tick bite. Water retention due to the SYNDROME (active existence conflict caused by the fear) exacerbates the symptoms. However, the same symptoms also occur as a consequence of earlier conflicts such as a motor conflict of not being able to escape, a “feeling soiled” conflict, or a self-devaluation conflict that are later diagnosed as borreliosis on the assumption that a tick bite could be the cause. The Lyme disease antibody test used to determine borreliosis is not only inconclusive. The test is also unable to explain why the "borreliosis" symptoms differ from person to person.
| |
In measles, rubella (also known as German measles), and chickenpox the skin rash covers most of the body. Generalized separation conflicts, which affect the entire body, are typically experienced by infants and young children who are much more vulnerable regarding separations from the “pack” (at home, at school). How the “childhood disease” presents itself depends on which epidermal layer is involved (chickenpox goes deeper than measles and rubella) and on the intensity of the preceding conflict-active phase (rubella causes milder symptoms than measles). With the SYNDROME, that is, with water retention as a result of an active abandonment conflict, the blisters of the skin rash appear more dramatic. An intense healing phase is accompanied by high fever.
 | Scarlet fever occurs when the separation conflict affects the underside of the epidermis (showing as white patches – see vitiligo) and the upper side of the epidermis with the development of a skin rash after the conflict has been resolved. A red and swollen tongue (“raspberry tongue”) indicates an additional “oral conflict” (possibly food-related); a “strep throat” points to a conflict of “not wanting to swallow a morsel” (food or, figuratively, a situation that is “hard to swallow”). The theory that the skin rash in scarlet fever is a “streptococcus infection” is, from a GNM point of view, irrelevant.
|
Based on the understanding of the Fourth Biological Law, these “childhood diseases” are not “contagious viral infections”, as claimed, but the healing phase of separation conflicts experienced by more children at the same time (the existence of viruses that supposedly cause measles, rubella, or chickenpox has never been scientifically substantiated – see GNM Article “Measles Virus put to the Test”). Such collective separation conflicts can be school-related (a separation associated with a schoolmate or teacher) or home-related affecting all siblings. In young children, measles occurs typically in the fall, after the child has become familiar with the (kindergarten) teacher and is accustomed to being picked up by mom daily after school. The skin rash is the visible sign that the separation conflict has been resolved. If the pediatrician knows that the child is not vaccinated, a measles diagnosis is much more likely. Not being allowed or not wanting to have contact with someone who has the “infection” results in a “spreading” of separation conflicts rather than of the condition itself. Measles outbreaks in school or among a larger population are often linked to the fear of coming in contact with an “infected” person.
 | This diagram shows the measles death rates in Germany between 1961 and 1995. Source: Federal Statistics Office Wiesbaden, Germany
The measles vaccination program started in 1976, well after the peak of the measles epidemic (see also polio vaccination program and tetanus vaccination program).
|
Psoriasis involves two separation conflicts; one is in the conflict-active phase causing a flaky skin, the other is in the healing phase showing as an inflammation. The two phases overlap at the same area(s), presenting as silvery scales on a thick, red surface. The location reveals which part of the body was associated with the conflict. What is termed “psoriatic arthritis” is, in GNM terms, a combination of separation conflicts and self-devaluation conflicts (see joints) that occurred simultaneously.
 | This picture shows psoriasis on both elbows indicating two localized separation conflicts of wanting to push someone away in defense (or wanting to get some “elbow room”) related, let’s say, to a terrorizing colleague at work and simultaneously to an annoying family member at home. The exact appearance of the condition is determined by which one of the two conflicts is active or healing at the time.
Psoriasis affects the two upper layers of the epidermis, namely the granular layer where squamous epithelial cells are converted into keratin and the stratum corneum where the buildup of keratin forms white plaques on the surface of the skin.
|
 | Herpes (here, a close-up image) presents as small, fluid-filled blisters similar to dermatitis or chickenpox. They develop at the area of the skin that correlates to the separation conflict, for example, on the lips (missing to be kissed or not wanting to be kissed, oral sex-related distress, lip contact with a dirty glass or an “infected” straw, cigarette “withdrawal”).
|

 | Herpes on the left cheek reveals that the separation conflict was associated with a partner, if the person is left-handed. For a right-handed person, it indicates a mother or child-related conflict.
A localized separation conflict translates into being touched at this particular area of the skin at the moment when the DHS occurred.
|
 | This brain CT shows fluid accumulation (in PCL-A) in the area of the right sensory cortex from where the epidermis of the left side of the face is controlled (view the GNM diagram). Hence, the development of a skin condition in this particular area.
|
Genital herpes on the external genitals (vulva, labia, penis, scrotum) or in the vagina are linked to a sexual separation conflict (loss of a sexual mate, sexual rejection, unwanted sex, sexual abuse). The fear or suspicion that a sexual mate might sleep with someone else can already trigger the conflict. The healing phase could also manifest as dermatitis on the genitals or as genital warts. Skin lesions on the genitals (male and female) might be diagnosed as a soft chancre (ulcus molle) or chancroid. In conventional medicine, it is considered the “first sign” of syphilis.
Venereal diseases are generally assumed to be bacterial or viral infections that “spread through sexual contact”. Yet, to this day, the existence of disease-causing viruses (herpes simplex virus, herpes zoster virus, HIV, HPV, and the like) has never been scientifically proven! Apart from that, based on the knowledge of the Five Biological Laws, venereal diseases such as gonorrhea, chancroid, syphilis, genital herpes as well as candidiasis (see penile candidiasis or vaginal candidiasis) and cancers involving the sexual organs (see cervical cancer) cannot be sexually transmitted since the symptoms are already healing symptoms. Hence, a sexual partner can only get, for example, herpes if he/she suffered a separation conflict at the same time, let’s say, because of imposed sexual abstinence based on the belief that the condition is contagious. The fear of having contracted a “sexually transmitted disease” could also activate a separation conflict. The distress experienced through unwanted sexual practices or forced prostitution explains why the prevalence of “venereal diseases” is higher among particular groups and populations.
 | A basalioma or basal cell carcinoma (left picture) arises from the basal layer of the epidermis that consists mainly of pigment-producing melanophores. Hence, the brownish color of the growth. A squamous cell carcinoma (right picture) originates in the upper layer of the epidermis. Both occur during the healing phase of a separation conflict. In conventional medicine, they are erroneously thought to be “skin cancers” caused by prolonged exposure to sunlight (see also melanoma).
|
 | So-called mollusca contagiosa are raised, pink or flesh-colored papules with a dimple in the center. The condition is allegedly caused by the “molluscum contagiosum poxvirus” and, as the name implies, thought to be a contagious infection, transmitted via physical or sexual contact (see venereal diseases). The location of the wart-like growths (face, neck, trunk, extremities, genitals) is determined by which area of the body the separation conflict was associated. The virus theory is unable to explain why the condition appears on a certain part of the skin, for example, on the outer right thigh (see picture).
|
Warts are the result of excessive healing due to continuous conflict relapses. They develop alone or in groups at the area of the skin that was associated with the separation; they appear raised or flat depending on the intensity of the recurring conflict. Skin tags, which are small flaps of tissue that hang off the skin by a connecting stalk, are similar to warts. Genital warts (condyloma) on the external sexual organs, in the vagina, in the cervix uteri, or on the penis reveal persistent sexual separation conflicts. Anal warts develop in or around the anus (compare with hemorrhoids related to the rectum surface mucosa). In conventional medicine terms, a small “wart-like growth” is called a papilloma or “benign epithelial tumor” (see also intraductal papilloma).
 | Plantar warts originate in the deep basal layer of the epidermis. They typically occur on the sole (Latin: planta) or toes of the feet. Wanting to “separate” from the ground one is standing on or, the opposite, namely not wanting to leave a place (workplace, sports facility, home, village, town, country) is the underlying conflict experience. Cats and dogs develop warts as well, for example, because of an unwanted move. Shoes such as work boots or hiking shoes one wants to get off, also lead to plantar warts, particularly at pressure points. The same applies to a clavus, commonly called a “corn”. The claim that plantar warts, unlike corns, are caused by the “contagious human papilloma virus (HPV)” has no scientific basis.
|
 | A lasting, intense healing phase (hanging healing) leads over time to a hardening of the skin or scleroderma, locally or throughout the body (generalized). Scleroderma can also involve the connective tissue layer underneath the skin. Often, the two Biological Special Programs (separation conflict and self-devaluation conflict) run concurrently.
|
SKIN - TRANSLATIONS
Click on the icon to download the PDF file
| |||||||||||||



{kind=link}
{kind=link}
{kind=link}