
ESOPHAGUS
 DEVELOPMENT AND FUNCTION OF THE ESOPHAGUS (LOWER THIRD): The esophagus is located behind the trachea and the larynx. Originally, the entire alimentary canal – from the mouth to the rectum – served the absorption (absorptive quality) and digestion (secretory quality) of food. Today, the main function of the esophagus is to carry food, liquids, and saliva from the mouth to the stomach. The act of swallowing is facilitated by the peristaltic movement (motor quality) of the smooth muscles in the esophagus (the upper two-thirds of the esophagus are mainly made up of striated muscles). The deep esophagus mucosa consists of intestinal cylinder epithelium, originates from the endoderm and is therefore controlled from the brainstem.
BIOLOGICAL CONFLICT: The biological conflict linked to the lower esophagus is “not being able or not being allowed to swallow a morsel”.
This type of morsel conflict relates to a “morsel” one had expected (a job, a promotion, a position, a deal, a purchase, an inheritance, a gift, an apology, a proposal) but is unexpectedly not able to get. A promise that has not been kept, something of personal value that has been taken away, projects or plans one is unable to carry out are other examples of what could evoke the conflict. A “morsel” one is unable to “swallow” could also concern a new relationship or a specific person such as a tenant, an employee, or a friend one had to give up. A desired “morsel” one is not allowed to get could also relate to a specific (favorite) food.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase esophageal cells proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to be better able to absorb and digest the desired morsel. Even though the esophagus has no longer a digestive function, in the event of a biological conflict the organ still responds with cell augmentation, because originally the entire alimentary canal served the absorption and digestion of food. With prolonged conflict activity (hanging conflict) a cauliflower-shaped growth (secretory type), referred to as an esophageal cancer, develops in the lower esophagus (compare with “esophageal cancer” related to the upper two-thirds). The tumor might also grow on a flat plane (absorptive type). If the rate of cell division exceeds a certain limit, conventional medicine considers the cancer as “malignant”; below that limit, the growth is regarded as “benign” or diagnosed as an esophageal polyp (see also healing phase).
It is assumed that an esophageal cancer is linked to gastric reflux. No question, the backflow of stomach acid might irritate the esophagus but this does not cause a “cancer”. In GNM terms, cell proliferation in the esophagus only occurs in response to the correlating biological conflict, namely to “not being able to swallow a morsel”. Gastric reflux, on the other hand, originates in the stomach and is related to a territorial anger conflict.
Esophageal spasms occur during the Epileptoid Crisis (see also esophageal spasms related to the upper two-thirds of the esophagus).
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. Healing symptoms are pain behind the sternum due to the swelling, and night sweats. A large swelling could constrict the esophagus with difficulties swallowing solid foods. With an acute narrowing, a feeding tube may have to be used until the tumor has been decomposed, provided the necessary microbes are available when healing sets in. Esophageal candidiasis indicates that fungi assist healing.
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells remain. Eventually, the growth becomes encapsulated with connective tissue. In conventional medicine, this is usually diagnosed as an esophageal polyp or as a “benign cancer” (see also conflict-active phase).
With the SYNDROME, that is, with water retention brought on by an active abandonment or existence conflict, the retained water is exceedingly stored in the healing area, which increases the swelling. If the swelling becomes very large, this could lead to a serious situation, because the pressure that occurs during an intense Epileptoid Crisis might break blood vessels causing severe bleeding into the intestine (tar stool) and vomiting blood.
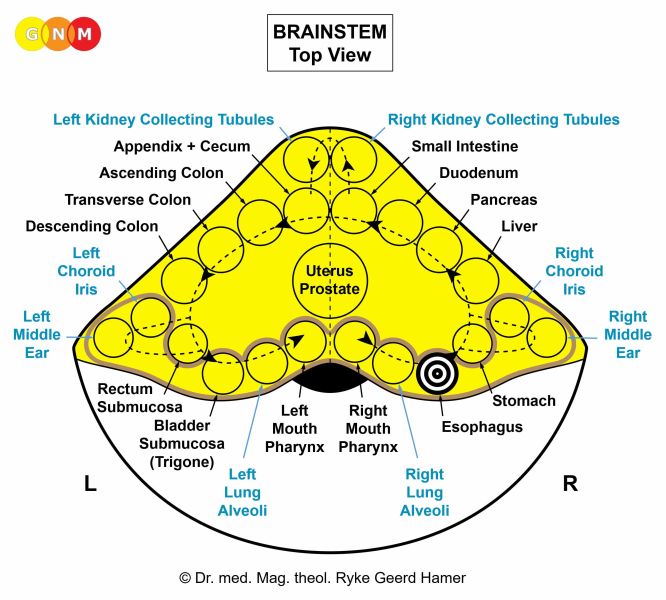
Esophageal “varices”: According to conventional medicine, esophageal varices are swollen veins in the lining of the lower esophagus. They are associated with liver cirrhosis and high blood pressure in the portal vein. Based on GNM, the swellings are in reality pouches in the esophagus lining (similar to diverticula in the intestines resulting from recurring repair processes). Moreover, the veins (new mesoderm) and the lower esophagus lining (endoderm) are different tissue types that derive from different embryonic germ layers and are therefore controlled from different areas in the brain. Hence, every person who has esophageal varices shows – without exception – the Hamer Focus in the brainstem, precisely, in the control center of the lower third of the esophagus (view the GNM diagram), and not in the cerebral medulla from where the blood vessels are controlled (see also the theory suggesting that hemorrhoids are swollen veins in the rectum).
|
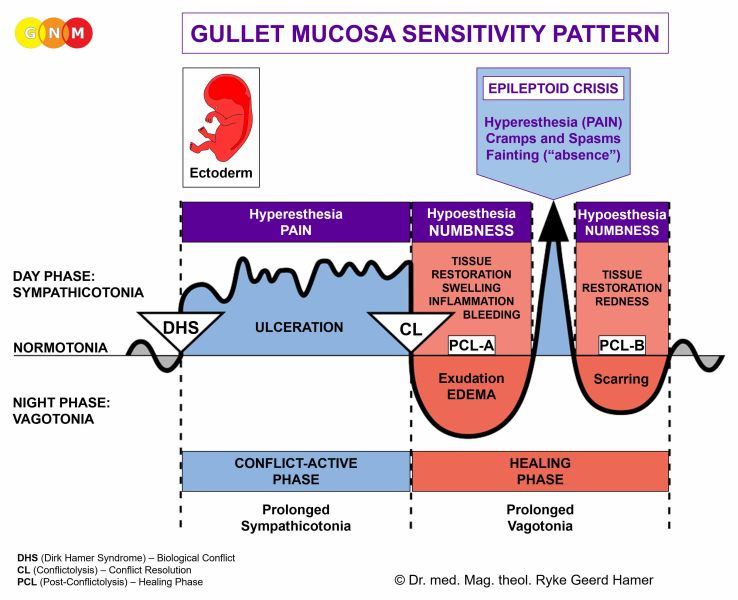
 DEVELOPMENT AND FUNCTION OF THE ESOPHAGUS (UPPER TWO-THIRDS): Originally, the inner wall of the entire esophagus consisted solely of intestinal cells (cylinder epithelium). At a later evolutionary stage, the endodermal lining of the upper portion of the esophagus was replaced with a new cell layer composed of squamous epithelium. However, clusters of endodermal cells remained also in the upper part. The epithelial lining of the upper two-thirds of the esophagus originates from the ectoderm and is therefore controlled from the cerebral cortex.
BIOLOGICAL CONFLICT: While the lower third of the esophagus is linked to “not being able to swallow a morsel”, the biological conflict associated with the upper two-thirds is the opposite, namely, “not wanting to swallow a morsel” (see also pharynx and throat). It is a type of “separation conflict”. This refers to any incident or situation one refuses to accept or words (accusations, insults, reproaches, criticism) that are difficult to “take” or hard to “swallow”. The unwanted morsel can also concern real food or medication.
CONFLICT-ACTIVE PHASE: ulceration in the lining of the upper esophagus proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the diameter of the esophagus to be better able to eliminate the undesirable “morsel”. Since the esophageal squamous epithelium is rather thick, it can take some time before deep ulcers are detected through an esophagoscopy. Symptoms: mild to severe pain. The typically burning pain is often misinterpreted as heartburn or “gastroesophageal reflux”.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation. In conventional medicine, this might be diagnosed as an “esophageal cancer” (compare with esophageal cancer related to the lower third of the esophagus). According to the Five Biological Laws, the new cells cannot be regarded as “cancer cells” since the cell increase is, in reality, a replenishing process.
Healing symptoms are difficulties swallowing because of the swelling and pain, which could last throughout the entire healing phase (in PCL-A and PCL-B the pain is not of a sensory nature but rather pressure pain). Concurrent water retention due to the SYNDROME enlarges the swelling. With an inflammation, the condition is called esophagitis. The Epileptoid Crisis manifests as acute burning pain.
|

 DEVELOPMENT AND FUNCTION OF THE ESOPHAGEAL MUSCLES: The esophagus is a muscular tube composed of smooth muscles in the lower part and striated muscles in the upper two-thirds. The tension of the muscles stabilizes the esophagus and allows swallowing and the transition of food. The esophagus is surrounded by two muscular rings, known as the esophageal sphincters. The opening of the upper esophageal sphincter is triggered by the swallowing reflex. The lower esophageal sphincter, also known as the cardiac sphincter, surrounds the lower part of the esophagus. At the level of the cardia, the opening connecting the esophagus with the upper part of the stomach, the esophagus rotates on its axis and thereby forms an elastic, twisting occlusion which contributes to the function of the sphincter, namely to open in order to allow food pass into the stomach and to close to keep it there. NOTE: The esophageal sphincters are functional but not anatomical sphincters like the bladder sphincter, anal sphincter, or cervical sphincter. The smooth esophageal muscles derive from the endoderm and are controlled from the midbrain. The striated esophageal muscles originate from
the new mesoderm and are controlled from the cerebral medulla and the motor cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the upper esophageal muscles is “not being able to regurgitate a morsel”, literally or figuratively (insult, accusation, diagnosis) because the morsel is considered too big.
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of esophageal muscle tissue (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing paralysis of the esophageal muscles (controlled from the motor cortex) causing difficulties swallowing foods and liquids.
HEALING PHASE: During the healing phase, the esophageal muscles are reconstructed. The paralysis reaches into PCL-A. The Epileptoid Crisis presents as esophageal spasms (see also esophageal spasms in the lower third of the esophagus). Depending on the degree of the conflict-active phase, the contractions range from mild to severe. During PCL-B, the function of the esophagus muscles returns to normal. Recurring esophageal spasms indicate a hanging healing due
| ||||||||||||||||||



