DEVELOPMENT AND FUNCTION OF THE PHARYNGEAL DUCTS: The pharyngeal ducts reach from the front and back of the ears into both sides of the neck further into the mediastinum, which is the middle section of the chest cavity containing the lungs, the heart, the esophagus, and the trachea. The lining of the pharyngeal ducts consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
|
| NOTE: The pharyngeal ducts developed at a time when life existed only in the ocean. In fish and amphibians they are equivalent to the gills, the respiratory organs that extract oxygen from water. The pharyngeal ducts are descendants of the pharyngeal arches (see also coronary arteries, coronary veins, aorta, carotid arteries, and subclavian arteries that derive from the pharyngeal arch arteries). In the embryo, the pharyngeal arches, or branchial arches (Greek branchial = gill), give rise to structures of the head and neck (see also thyroid ducts). In humans, the pharyngeal ducts develop during the fourth week of gestation.
|
|
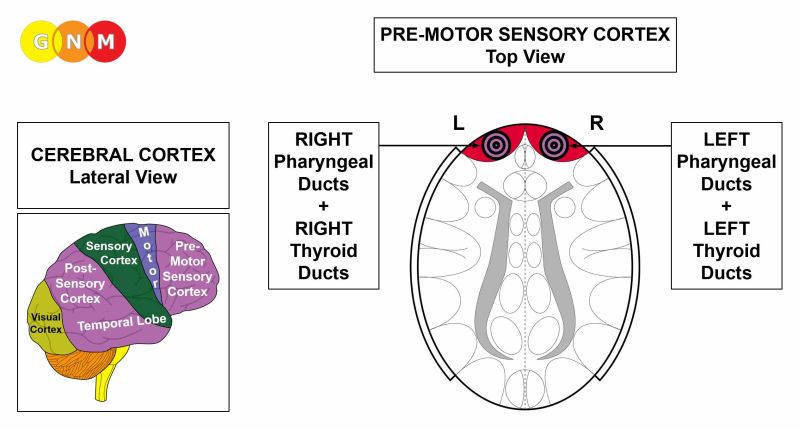
| BRAIN LEVEL: The epithelial lining of the pharyngeal ducts is controlled from the pre-motor sensory cortex (part of the cerebral cortex). The left pharyngeal ducts are controlled from the right side of the cerebral cortex; the right pharyngeal ducts are controlled from the left cortical hemisphere (frontal). Hence, there is a cross-over correlation from the brain to the organ.
NOTE: The pharyngeal ducts and thyroid ducts share the same brain relays. The DHS affects either one of the tissues or both, depending on the intensity of the conflict.
|
Gender, Laterality, Hormone Status
| Biological Conflict
| Affected Organ
|
|
|
| |
| Frontal-fear conflict
| Left pharyngeal ducts
| |
| Frontal-fear conflict
| Right pharyngeal ducts*
| |
|
| Right pharyngeal ducts
| |
|
| Left pharyngeal ducts*
|
|
|
| |
|
| Right pharyngeal ducts
| |
|
| Left pharyngeal ducts*
| |
| Frontal-fear conflict
| Left pharyngeal ducts
| |
| Frontal-fear conflict
| Right pharyngeal ducts*
|
NHS = Normal hormone status LTS = Low testosterone status LES = Low estrogen status
*With left-handers the conflict is transferred to the other brain hemisphere
|
A frontal-fear conflict is a big fear of heading into a dangerous situation or of danger that is moving directly towards one. The conflict can be experienced in real terms, for example, during a head-on accident or a frontal attack by a person or an animal. In a transposed sense, the approaching danger could be a threatening confrontation, for example, with a government agency or the banks. A frontal-fear might be prompted by unexpected shocking news that are perceived as a “blow in the face”. Often, the conflict is triggered by follow-up examinations or the announcement of a medical procedure such as surgery. One of the most common frontal-fear conflicts is being faced with a cancer diagnosis. In GNM, we therefore call the conflict related to the pharyngeal ducts also a “cancer fear conflict”.
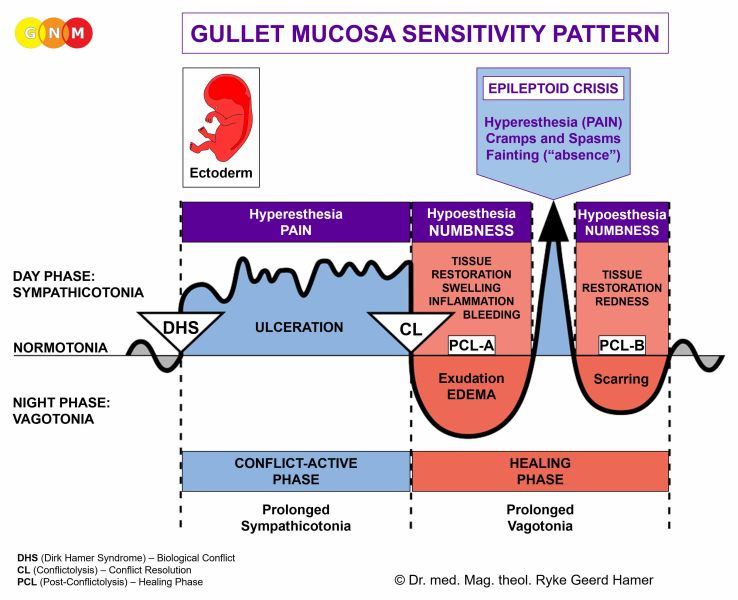
CONFLICT-ACTIVE PHASE: ulceration in the lining of the pharyngeal duct proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the ducts to allow more oxygen intake, even though in humans the pharyngeal ducts have no longer a respiratory function. Symptoms: mild to severe pain in the neck area.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation with swelling due to the edema (fluid accumulation) in the healing area. The swelling might be diagnosed as mononucleosis or Pfeiffer’s disease (compare with mononucleosis related to the lymph nodes). Whether the swelling occurs in the pharyngeal ducts or in the lymph nodes can be easily established with the help of a brain CT that shows the impact of the related conflict in the corresponding brain relay. In addition, if the lymph nodes are affected the lymphocyte count is elevated, which is not the case with a healing process in the pharyngeal ducts.
A hanging healing due to continuous conflict relapses leads to the back-up of fluid in the affected duct resulting in the development of a cyst located laterally on the right or left side of the neck or collarbone area (compare with thyroid cysts located towards the middle) or in the mediastinum where it is called a retrosternal struma. After the Epileptoid Crisis, the cyst recedes parallel to the completion of the healing process. However, if the healing phase cannot be complete, the cyst hardens and stays.
|
| A cyst in the pharyngeal ducts (shown in this picture on the left side of the neck) is often diagnosed as a non-Hodgkin’s lymphoma, based on the wrong assumption that the “tumor” develops in the cervical lymph node (compare with Hodgkin's lymphoma and non-Hodgkin's lymphoma associated with lymphocytic leukemia).
In conventional medicine, embryology has no clinical relevance. Hence, in the medical practice, the pharyngeal ducts have been completely ignored.
|
|
|
This brain CT shows an accumulation of neuroglia in the control center of the left pharyngeal ducts ( view the GNM diagram), indicating that the person has already passed the Epileptoid Crisis and is now in PCL-B of the healing phase (both on the brain and on the organ level). In conventional medicine, the glia buildup is erroneously believed to be a “brain tumor”.
|
Found in the mediastinum, a cyst in the pharyngeal ducts is diagnosed as a “small cell bronchial carcinoma” or “small cell lung cancer” (see also mediastinal osteosarcoma). In the mediastinum, a large cyst might compress vital vessels or cause breathing difficulties due to the pressure on the trachea with acute shortness of breath and choking fits during the Epileptoid Crisis, when the fluid in the cyst is expelled. With the SYNDROME, that is, with water retention as a result of an active abandonment or existence conflict (diagnosis shock, hospitalization) the situation could become critical.
PHARYNGEAL DUCTS - TRANSLATIONS
|
| <---- In these PDF documents you can enlarge images. If your browser cannot handle this desirable feature, then you will need to download and install the authentic Adobe Acrobat Reader. |
Click on the icon to download the PDF file
|
English Original
|
Catalan Translation
|
Dutch Translation
|
|
French Translation
|
Hungarian Translation
|
Russian Translation
|
|
Serbian Translation
|
Spanish Translation
|
Turkish Translation
|
|
|