
EYES
 DEVELOPMENT AND FUNCTION OF THE TEAR GLANDS: The tear glands are located in the temporal orbit (eye socket) on the outer portion of the upper eyelids. They produce the watery layer of the tear film that keeps the outer part of the eye and the conjunctiva moist. The tear fluid reaches the eye through the excretory tear ducts. Excess tears drain through the lacrimal canals, tear sac, and nasolacrimal duct into the nasal cavity. In evolutionary terms, the tear glands developed from the intestinal mucosa of the original gullet. Like the intestinal cells that digest the “food morsel”, the biological function of the tear glands is to “digest” (secretory quality) the “visual morsel”. The tear glands consist of intestinal cylinder epithelium, originate from the endoderm and are therefore controlled from the brainstem.
BIOLOGICAL CONFLICT: The biological conflict linked to the tear glands is a “morsel conflict”, specifically, a conflict related to a “visual morsel” (see also choroid, iris, and ciliary body).
RIGHT TEAR GLAND
LEFT TEAR GLAND
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the tear gland proliferate causing an enlargement of the lacrimal gland. The biological purpose of the cell increase is to enhance the production of tear fluid so that the “visual morsel” can be better absorbed (right tear gland) or expelled (left tear gland). Thus, the affected eye is teary and watering (see also nasolacrimal ducts and conjunctiva).
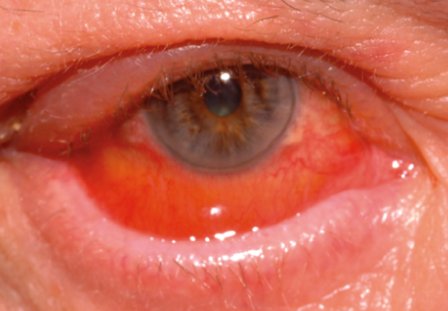
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. Healing symptoms are swelling of the tear gland caused by the edema (fluid accumulation) and purulent eye discharge. In PCL-B, the sticky pus dries up showing as yellowish eye crust around the eye(s). In conventional medicine, agglutinated and crusty eyelids are associated with “allergies” (see conjunctivitis).
The healing phase might be accompanied by an inflammation (dacryoadenitis) with redness and painful swelling of the lacrimal gland. With the SYNDROME, that is, with water retention as a result of an active abandonment or existence conflict, the swelling increases even more. The condition occurs quite often in children.
With a hanging healing due to constant conflict relapses more and more tear gland tissue is lost resulting in a decreased tear flow or a complete cessation of tear fluid production. The drying-up of the lacrimal flow (xerophthalmia) is termed Sjogren’s or Sicca syndrome (see also dry eyes related to the excretory tear ducts, eyelid gland ducts, conjunctiva, and Sjogren’s associated with a dry mouth).
|







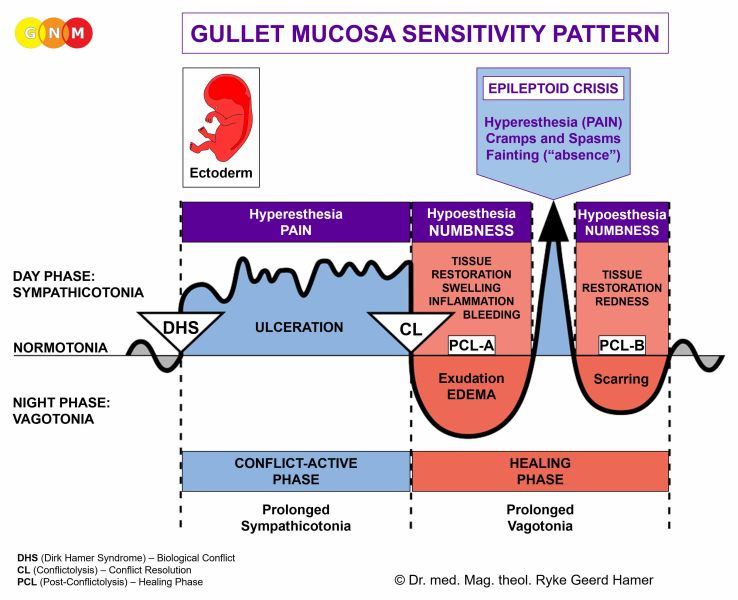
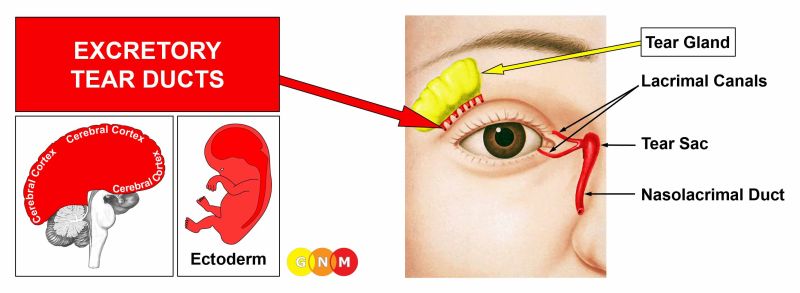 DEVELOPMENT AND FUNCTION OF THE TEAR DUCTS: The excretory tear ducts release the tear fluid produced by the tear glands into the top part of the conjunctiva and to the outer surface of the eyes. The lacrimal canals, which are two curved tubes located at the inner border of each eyelid, drain excess tears into the tear sac and through the nasolacrimal duct into the nasal cavity. The lining of the tear ducts consist of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
BIOLOGICAL CONFLICT: Similar to a separation conflict, the biological conflict linked to the tear ducts is “wanting to be seen” (not being noticed or overlooked, feeling visually ignored, not allowed to be seen) or “not wanting to be seen” (wanting to be invisible; a fear of getting caught, let’s say, in a criminal act, a sexual act, or when cheating).
CONFLICT-ACTIVE PHASE: ulceration in the epithelial lining of the tear ducts proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the ducts in order to increase the tear flow. The “shiny eyes” makes the one who has been overlooked more eye-catching (in Nature, this is vital to attracting a mate). Symptoms are teary eyes and potentially painful pulling in the affected tear duct. With an acute conflict the tearing could be excessive (see also watery eyes related to the tear glands and the conjunctiva).
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation with swelling due to the edema (fluid accumulation) in the healing area. Depending on the intensity of the conflict-active phase, the swelling could lead to an obstruction of the tear ducts causing dry eyes. A chronic condition because of continual conflict relapses is called Sjogren’s or Sicca syndrome (see also dry eyes related to the tear glands, eyelid gland ducts, conjunctiva, and Sjogren’s associated with a dry mouth). However, in this case, Sjogren’s is not preceded by a swelling of the tear glands. An occlusion of the excretory tear ducts leads to an enlargement of the entire tear gland. The swelling is therefore frequently misdiagnosed as a lacrimal gland tumor.
Blocked tear ducts are quite common in infants. In infants and newborns the condition reveals the distress of “wanting to be seen” (not getting enough attention) or “not wanting to be seen” (too many visitors stopping by to see the new baby).
If the nasolacrimal ducts are blocked, tears cannot empty into the nasal cavity. The back-up of tears results in watery and teary eyes. An obstruction of the nasolacrimal duct with swelling and redness in the area between the eye and the nose, including the lacrimal sac, is called dacryocystitis (“tear sac infection”).
|


 DEVELOPMENT AND FUNCTION OF THE EYELID GLANDS: The eyelids are movable folds of skin that cover and protect the eyes. The eyelashes attached to the upper and lower eyelids form a second protective shield against dust and other elements that could injure the eye. The outermost layers of the eyelid consist of epidermal tissue (outer skin) and fat tissue. Two eyelid muscles allow the opening and closing of the eyelids. The inside of the lids is lined with the conjunctiva. The main function of the eyelids is to keep the front surface of the eyeball and cornea moist. The meibomian glands and glands of Zeis are a special type of oil-producing sebaceous glands located at the rim of the upper and lower eyelids inside the tarsal plate. Close to the base of the eyelashes are also sweat glands, called the glands of Moll (both the sebaceous glands and sweat glands are embedded in the corium skin). The excretory ducts of the eyelid glands carry the oily sebum into the tear film to lubricate the eye during blinking. The eyelid glands originate from the old mesoderm and are therefore controlled from the cerebellum.
BIOLOGICAL CONFLICT: The biological conflict linked to the eyelid glands is an attack conflict, specifically, an attack against the eye (see also corium skin).
Dust, sand, or other particles (or a bug) hitting the eye can be registered as an attack conflict. In a figurative sense, the “attack” could be triggered by an insulting look (the “evil eye”) or a look of reproach. The conflict also relates to feeling disfigured, soiled or “dirty” concerning the eyelids. A “yucky” touch or kiss on the eye(s) might activate the conflict. Buying into the theory that touching the eyes after contact with a person who has a cold causes an “eye infection” only creates a predisposition for the conflict.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the eyelid glands proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to provide an external reinforcement in order to protect the eyelid against further “attacks”. If the conflict persists, a bulb-shaped growth forms at the site, possibly diagnosed as an eyelid tumor (compare with a melanoma of the eyelid involving the corium skin).
HEALING PHASE: Following the conflict resolution (CL), fungi or bacteria remove the cells that are no longer needed. During the healing process, the affected area swells up causing what is referred to as a stye (hordeola). The painful sore is red and filled with pus.
External styes involve the glands of Moll. They develop on the upper or lower lid margin at the base of the eyelashes. Internal styes relate to the meibomian glands and occur on the inside of the eyelid. If the meibomian glands become blocked and inflamed this results in a so-called chalazion (see right picture above), presenting as a granuloma that typically forms inside the upper eyelid. A chalazion is usually an indication of a hanging healing due to frequent conflict relapses. Feeling disfigured because of the appearance of the stye prolongs the healing phase.
If the required microbes are not available at the time, the additional cells remain. Eventually, the growth becomes encapsulated with connective tissue.
|




 DEVELOPMENT AND FUNCTION OF THE EYELID GLAND DUCTS: The excretory ducts of the eyelid glands are located along the margin of the upper and lower eyelid. They carry the oily substance (sebum) produced in the eyelid glands into the tear film to keep the eyes moist and prevent tears from evaporating too quickly. The eyelid gland ducts consist of squamous epithelium, originate from the ectoderm and are therefore controlled from the cerebral cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the eyelid gland ducts is a visual separation conflict experienced as having lost sight of someone, for example, of a loved one who has moved away, has left or has died (see also outer skin of eyelid, conjunctiva, cornea and lens). The conflict also relates to not being allowed or not wanting to see someone (a specific person or certain people). NOTE: A visual separation conflict only refers to people and animals such as a pet but not to objects (ring, car, favorite toy) or a home. This would instead involve the tear glands or the uvea of the eye.
CONFLICT-ACTIVE PHASE: ulceration in the eyelid gland ducts proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the ducts to increase the flow of lipids to keep the eye lubricated. In Nature, the clearer vision allows to quickly recognize a new mate that “strikes the eye”.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation with swelling due to the edema (fluid accumulation) in the healing area. The swelling might occlude the ducts (called “Meibomian gland dysfunction”). The blockage leads to a thinning of the lipid tear film layer and increased evaporation of tears causing dry eyes. If the symptom becomes chronic because of conflict relapses, then the condition is termed Sjogren’s or Sicca syndrome (see also dry eyes related to the tear glands, excretory tear ducts, conjunctiva, and Sjogren’s associated with a dry mouth).
|

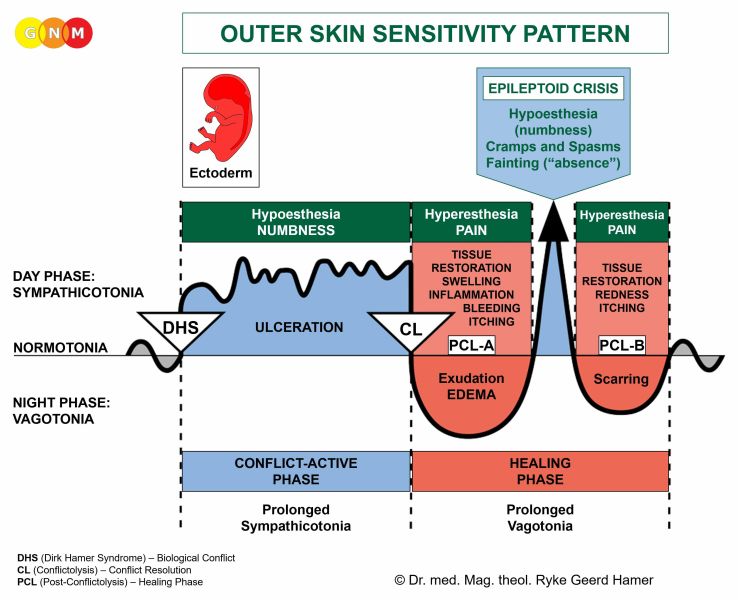
 DEVELOPMENT AND FUNCTION OF THE EYELID SKIN (EPIDERMIS): The eyelid skin consists of two layers: the corium skin and the outer skin (epidermis). The inside of the eyelid is lined with the conjunctiva. The outer eyelid skin, which is relatively thin, is supported by the tarsal plate to which the eyelid muscles are attached. The outer skin of the eyelid consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the eyelid skin is a visual separation conflict, specifically, having lost sight of a person while one had the eyes closed. For example, a loved one left or died unexpectedly while one was asleep; a mother lost sight of her infant while she was dozing off (compare with visual separation conflict related to the eyelid gland ducts, conjunctiva, cornea and lens). The outer skin (epidermis) of the eyelids also relates to a loss of physical contact associated with the eyes, for example, being no longer kissed on the eyelids (see separation conflict) as well as wanting to separate from something or someone that touches the eyes (an unwanted kiss on the eyelid, being blindfolded, “toxic” eye makeup).
CONFLICT-ACTIVE PHASE: ulceration in the epithelial lining of the eyelid skin proportional to the degree of conflict activity. The ulcerative process makes the eyelid skin dry and flaky. When the lower eyelid is involved, the area below the eye is also affected. The Biological Special Program of the outer skin is always accompanied by a short-term memory loss, which serves the purpose to forget temporarily the one who is absent, here, specifically, the one who is out of sight.
HEALING PHASE: During the healing phase (in PCL-A) the ulcerated area is replenished with new cells. With an inflammation the condition is called blepharitis. The symptoms, including swelling, redness, a burning sensation and itching, range from mild to severe, depending on the intensity of the conflict-active phase.
|





 DEVELOPMENT AND FUNCTION OF THE EYELID MUSCLES: The eyelids contain three main muscles that control the movement of the eyelid. The two muscles involved in opening the upper eyelid are the levator palpebrae muscle (for voluntary opening) and the superior tarsal muscle (for involuntary opening). The orbicularis oculi muscle in the upper and lower eyelid controls the closing of the eye. As the eye elevates the levator muscle contracts and raises the eyelid; when the levator relaxes, the eyelid closes passively. Active eyelid closure to protect the eyes from injury and from excessive light (see pupil muscles) is achieved by the contraction of the orbicularis oculi. The eyelid muscles also control the blink reflexes. Blinking provides moisture to the eyes and the cornea by using tears (produced in the tear glands) and oily substances (secreted by the eyelid glands) to keep it from drying out. The eyelid muscles are attached to the tarsal plate that gives the eyelids shape and strength. The levator palpebrae and orbicularis oculi consist of striated muscles, originate from the new mesoderm and are controlled from the cerebral medulla and the motor cortex. The superior tarsal muscle is a smooth muscle.
LEVATOR PALPEBRAE MUSCLE
BIOLOGICAL CONFLICT: The biological conflict linked to the levator palpebrae muscle is not being able to keep the eye(s) open (because of extreme fatigue, working night shifts) or not having kept the eye(s) open (having been wide awake) at the right time (having missed a red traffic light or an important visual message, e.g., on a blackboard or screen; having overlooked something of importance such as the small print of a contract). Certain professions, for example, policemen, detectives, pilots, professional drivers, people attending monitors and other devices used for observation are more susceptible to suffer this type of conflict. The levator muscle also relates to not being allowed to keep the eye(s) open (being prohibited to see or watch something) or not wanting to keep the eye(s) open (wanting to avoid seeing something distressing).
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of the levator palpebrae (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing paralysis of the levator muscle (controlled from the motor cortex).
Because of the weakness or paralysis of the levator muscle, responsible for raising the eyelid, the upper eyelid sags and fails to fully open. Depending on the intensity of the conflict, the droop may be barely noticeable or the eyelid can descend over the entire pupil. Yet, the eyelid doesn’t close to cover the eye completely since the tarsal muscle prevents a complete closing. In medical terms, a drooping eyelid is called blepharoptosis (or ptosis). The inability to fully close the eyelid is termed lagophthalmos.
HEALING PHASE: During the healing phase the levator muscle is reconstructed; the paralysis reaches into PCL-A. The Epileptoid Crisis manifests as eyelid muscle spasms (blepharospasm). Depending on the degree of the conflict-active phase, the rapid movement of the eyelid ranges from minor eyelid fluttering to strong eyelid twitching or eyelid tics (compare with facial tics). In PCL-B the function of the eyelid muscle returns to normal.
Excessive eye blinking also involves the levator muscle. The explicit conflict linked to the blink reflex is feeling sussed out or figured out, for example, when someone was caught cheating, lying, or playing tricks. The rapid blinking occurs during the Epileptoid Crisis and is typically triggered when setting on a track, for example, when the person is telling a lie.
ORBICULARIS OCULI MUSCLE
BIOLOGICAL CONFLICT: The biological conflict linked to the orbicularis oculi muscle is not being able to close the eyes (in order to avoid seeing something unpleasant or undesirable; wanting to turn a “blind eye” to something) or not having closed the eyes at the right time (accidents caused by exposure to fire or explosives or by unsafe work with a welding device). The orbicularis oculi also relates to not being allowed to close the eyes (not being permitted to sleep or not getting enough sleep, for example, mothers with newborns, students working on last-minute term papers, shift workers, long-distance truck drivers) or not wanting to close the eyes (kids refusing to nap).
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of the orbicularis oculi of the upper or lower eyelid (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing paralysis of the orbicularis oculi muscle (controlled from the motor cortex).
Because of the weakness or paralysis of the orbicularis oculi muscle, responsible for closing the eyelid, the upper and lower eyelid cannot be closed properly (see also facial paralysis with the inability to close the eye on the paralyzed side. The orbicularis oculi and the facial muscles are both supplied by the facial nerve).
HEALING PHASE: During the healing phase the orbicularis oculi muscle is reconstructed; the paralysis reaches into PCL-A. The Epileptoid Crisis manifests as eye muscle spasms (blepharospasm) of the upper or lower eyelid. Depending on the degree of the conflict-active phase, the rapid movement of the eyelid ranges from minor eyelid fluttering to strong eyelid twitching or eyelid tics (see also facial tics). In PCL-B the function of the eyelid muscle returns to normal.
|




 DEVELOPMENT AND FUNCTION OF THE CONJUNCTIVA, CORNEA, AND LENS: The conjunctiva is a clear mucous membrane that lines the sclera (the white of the eye) and the inside of the eyelid. The main function of the conjunctiva is to produce tears to keep the front surface of the eyeball moist. The larger volume of tear fluid, however, is secreted by the tear glands. The cornea is a transparent structure that covers the iris and the pupil. The cornea controls the entry of light into the eyes. When light strikes the cornea, it refracts the incoming light onto the lens that refocuses the light onto the retina. The crystalline lens is located behind the iris and held in place by the ciliary muscles that allow altering the shape of the lens in order to get sharp images of objects at various distances. Both the cornea and the lens are responsible for the eye’s focusing power and for fine-tuning the vision process. The conjunctiva, cornea, and lens consist of squamous epithelium, originate from the ectoderm and are therefore controlled from the cerebral cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the conjunctiva, cornea, and lens is a visual separation conflict of having lost sight of someone, for example, of a loved one who has moved away, left, or has died (see also eyelid gland ducts and outer skin of eyelid). This includes having lost sight of a pet. The conflict also relates to not being allowed to see someone (a grandchild, a lover, a friend, a schoolmate, a relative in the hospital) or not wanting to see someone (“get out of my sight!”). The fear of not being able or not being permitted to see a certain person might already trigger the conflict. The degree of the conflict determines which one of the three tissues will be affected by the DHS. The conjunctiva is associated with a light visual separation conflict, the cornea with a moderate conflict; the lens is affected when the conflict is experienced as severe. NOTE: A visual separation conflict only refers to people and animals such as a pet but not to objects (ring, car, favorite toy) or a home. This would instead involve the tear glands or uvea of the eye.
CONFLICT-ACTIVE PHASE: ulceration in the conjunctiva, cornea, or lens. In the lens, the loss of crystalline cells improves the reception of light and therefore the visual acuity with the biological purpose that the person fading from one’s sight will be longer visible. The enhanced distant vision also increases the chance of detecting a lost “pack member” in the far distance. The Biological Special Programs of the conjunctiva, cornea, and lens are accompanied by a short-term memory loss, which serves the purpose to forget temporarily the one who is out of sight (see separation conflict related to the skin).
In the conjunctiva, the ulceration makes the eye(s) dry (see also dry eyes related to the tear glands, excretory tear ducts, and eyelid gland ducts).
If the cornea’s angle of curvature becomes too steep, this causes nearsightedness or myopia (see also smooth ciliary muscles and retina). Farsightedness or hyperopia occurs when the cornea has too flat of an angle (see also striated ciliary muscles and retina).
HEALING PHASE: During the healing phase the cell loss is restored and replenished.
According to conventional medicine, cataracts are considered a normal part of the aging process even though not every person develops a cataract at an older age. From a GNM point of view, it is rather the increasing incidences of visual separation conflicts – from a parent, a spouse, a long-time companion or friend – why cataracts are much more common in older people.
In the cornea, the healing symptom presents as blurry vision. With an inflammation the condition is called keratitis. Symptoms are pain and redness. With constant conflict relapses an astigmatism (see conflict-active phase) becomes permanent due to recurrent scarring processes in the cornea.
Conjunctivitis and chemosis are commonly associated with “allergies” and assumed to be caused by the exposure to pollen. With concurrent cold symptoms such as a runny nose, the “allergy” is called “hay fever”. In GNM terms, the combination of the symptoms is a sign that the healing phase of a visual separation conflict and of “scent or stink conflict” related to the nasal mucosa happen simultaneously. Agglutinated and crusty eyelids reveal that an additional “visual morsel conflict” involving the tear glands has also been resolved.
|
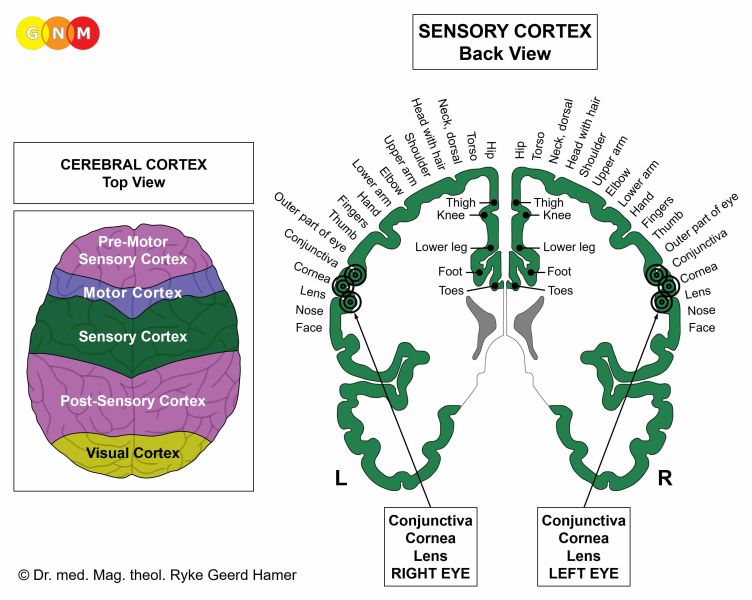







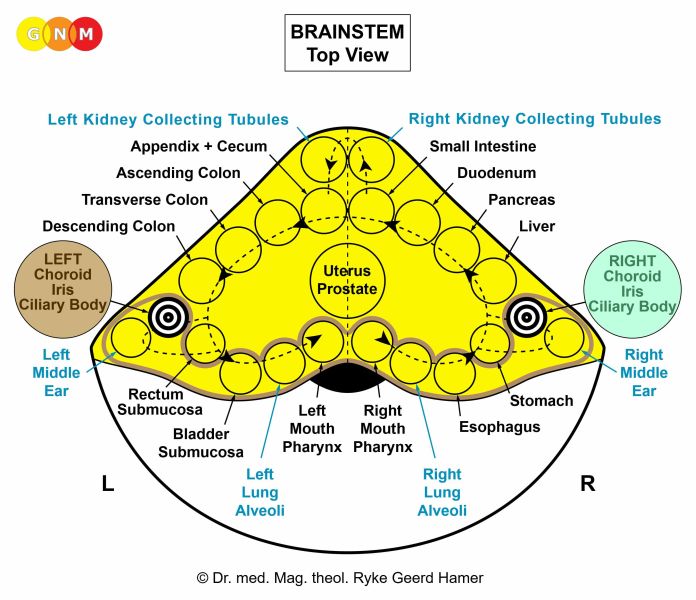
 DEVELOPMENT AND FUNCTION OF THE CHOROID, IRIS, AND CILIARY BODY: The choroid, iris, and ciliary body are collectively called the uvea. The choroid lines the inner surface of the eyeball and supplies the underlying retina with nutrition. The iris in the front of the eye is part of the choroid. The iris helps to regulate the amount of light that enters the eye (see also cornea) and is therefore functionally closely tied to the pupils. The ciliary body connects the choroid with the iris. The ciliary body produces a watery fluid (intraocular fluid or aqueous humor) that fills the anterior and posterior chamber of the eyeball. The function of the intraocular fluid is to maintain the intraocular pressure (see also vitreous body). The ciliary body contains the ciliary muscles that control the shape of the lens to allow clear vision. The uvea contains considerable amounts of melanin pigments to protect the eye from excess light (see also corium skin). In the iris, the quantity of melanin determines the color of the iris ranging from brown to blue. In evolutionary terms, the choroid, iris, and ciliary body constitute the primordial eyecup that developed from the intestinal mucosa of the original gullet (see also pupil muscles and ciliary muscles). Like the intestinal cells that absorb and digest the “food morsel”, the biological function of the uvea is to “absorb” (absorptive quality) and to “digest” (secretory quality) the “visual morsel”. The choroid, iris, and ciliary body consist of intestinal cylinder epithelium, derive from the endoderm and are therefore controlled from the brainstem.
BIOLOGICAL CONFLICT: The biological conflict linked to the choroid, iris, and ciliary body is a “morsel conflict”, specifically, a conflict related to a “visual morsel” (see also tear glands).
UVEA OF THE RIGHT EYE
In biological terms, the ingoing “visual morsel” is equal to nourishment (see also sound morsel related to the middle ear and Eustachian tubes). Figuratively speaking, the conflict experience is “I want to devour what I desire with my eyes”. What one is “drooling” to see can relate to anyone or anything one is not or no longer able to see or not allowed to see, for example, a beloved person or a home one had lost. It might also be about something one had anticipated to see (a certain person, paper money, a toy, a TV program, a vacation resort) and could unexpectedly not visually “grab” or “catch sight of”. The fear of becoming blind (“not being able to catch a visual morsel”) triggered, for example, by an MS diagnosis, a diabetes diagnosis (see diabetic retinopathy), or the negative prognosis of a macular degeneration could also prompt the conflict.
UVEA OF THE LEFT EYE
Such an undesired “visual morsel” relates to any “eyesore” one wants to get rid of (“I can’t bear to look at this”) or images one wants to erase from one’s memory. Eye-witnessing an accident or crime, seeing a spouse or partner with someone else, or watching something disturbing on TV can activate the conflict. Children suffer the distress when “catching” their parents or witnessing family abuse. The unwanted “visual morsel” could also be a person one does no longer want to see (a relative, parent, ex-spouse, “friend”, colleague, teacher, visitor).
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the choroid, iris, or ciliary body proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to be better able to absorb (right eye) or expel (left eye) the “visual morsel”. Which one of the tissues is affected is random.
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer required.
In the choroid, the tubercular lesions are visible as white spots behind the retina; they disappear with the completion of the healing phase. A continuous decomposing process, however, creates caverns in the choroid that are eventually filled with calcium deposits. The loss of pigmentation causes light sensitivity.
|







 DEVELOPMENT AND FUNCTION OF THE PUPIL MUSCLES: The pupil is the black round hole in the center of the iris. Its blackness is due to the lack of reflection of light from within the eye. The pupils consist of two muscles that regulate the amount of light that enters the eye. The dilator muscle widens the pupils allowing more light to pass through the eyes; the pupil sphincter narrows the pupils so that less light reaches the retina. In bright light the sphincter muscle contracts while the dilator muscle relaxes, making the aperture smaller. In dim light the sphincter muscle relaxes while the dilator muscle contracts, opening up the aperture. The dilator muscle is supplied by sympathetic nerves, which is why the pupils become large during stress (sympathicotonia) or sexual arousal. The pupil sphincter is supplied by parasympathetic nerves making the pupils small during relaxation (vagotonia). In evolutionary terms, the pupil muscles belong to the primordial eyecup that developed from intestinal cells (see also ciliary muscles and ciliary body). Like the intestinal muscles that move the “food morsel” along the intestinal canal through peristaltic motion, the pupil muscles contract and expand in response to the “light morsel”. The dilator muscle and pupil sphincter are composed of smooth muscles, derive therefore from the endoderm and are controlled from the midbrain.
BIOLOGICAL CONFLICT: According to their function, the pupil muscles are linked to a light-related morsel conflict – literally or figuratively.
The dilator muscle of the right pupil corresponds to the conflict of “not enough light to catch a morsel”. This can relate to any important information (on a board or screen), warnings (“watch your step!”), signs (a road sign) or a person that was overlooked because of insufficient light. The left pupil correlates to “not enough light to eliminate a morsel”, for example, if one is not able to avert a dangerous situation (an accident, an attack) because it was too dark (compare with the distress of sudden long darkness associated with the pineal gland). In a figurative sense, the conflict can be provoked if one is unexpectedly not in the “limelight” or not presented in the “proper light”.
The pupil sphincter of the right pupil corresponds to the conflict of “too much light to catch a morsel” (a visual morsel that is of importance), let’s say, because one was blinded by the sun or by bright light such as headlights, spotlights, a searchlight, a (police) flashlight, or a welding device. The left pupil correlates to “too much light to eliminate a morsel”, for example, if one is not able to prevent a dangerous situation because it was too bright. In a figurative sense, the conflict could be triggered when the “spotlight” is turned on someone, bringing something unpleasant or embarrassing “to light”.
CONFLICT-ACTIVE PHASE:
HEALING PHASE: During the healing phase the muscle tension goes back to normal. The Epileptoid Crisis presents as pupil spasms (compare with fluttering of the lens and nystagmus related to the extraocular muscles).
|




 DEVELOPMENT AND FUNCTION OF THE CILIARY MUSCLES: The ciliary body contains a set of ciliary muscles that regulate the changing of the lens shape (accommodation) to produce a clear vision at varying distances. Ligaments, called zonules, connect the ciliary body with the lens to hold it in place. The contraction of the ciliary muscles relaxes the zonules causing the lens to become rounder, which increases its power to focus on nearby objects. When the ciliary muscles relax, the zonules pull the edges of the lens making it flatter to see objects in a far distance. The ciliary muscles are composed of smooth muscles (involuntary) and striated muscles (voluntary). In evolutionary terms, the smooth ciliary muscles belong to the primordial eyecup (see ciliary body and pupil muscles); they therefore originate from the endoderm and are controlled from the midbrain. The striated ciliary muscles derive from the new mesoderm and are controlled from the cerebral medulla and the motor cortex.
SMOOTH CILIARY MUSCLES
BIOLOGICAL CONFLICT: The biological conflict linked to the smooth ciliary muscles is “not being able to see what is close” (difficulties reading small print, for example, in a newspaper, on a blackboard, computer screen, or phone screen), “not being allowed to see what is close”, or “not wanting to see what is close” (not wanting to see what takes place right in front of one’s eyes, e.g., family violence; wanting to play outside rather than doing homework).
CONFLICT-ACTIVE PHASE: sustained hypertonus (contraction) of the smooth ciliary muscles causing a relaxed tension on the zonules and subsequently a curved lens, which serves the biological purpose to be better able to see what is close. Ongoing conflict activity results in nearsightedness or myopia (see also cornea and retina). NOTE: Working with fine tools (needlework) or “staring at the screen all day” strains the focusing power of the ciliary muscles leading over time to nearsightedness – without a DHS.
HEALING PHASE: During the healing phase the muscle tension goes back to normal. The Epileptoid Crisis manifests as fluttering of the lens to which the ciliary muscles or rather the zonules are attached (compare with pupil spasms and nystagmus related to the extraocular muscles).
STRIATED CILIARY MUSCLES
BIOLOGICAL CONFLICT: The biological conflict linked to the striated ciliary muscles is “not being able to see what is in the distance” (a person or object is too far away to be recognized or identified; difficulties reading a sign because it is too far away) or “not being allowed to see what is far away” (not being permitted to visit someone or to go on a journey) but also “not wanting to see what is in the distance” (a person who is leaving).
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of ciliary muscles (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing paralysis (weakness) of the striated ciliary muscles (controlled from the motor cortex). This causes the zonules to tighten making the lens flat, which serves the biological purpose to be better able to see what is far away. Prolonged conflict activity results in farsightedness or hyperopia (see also lens and retina).
HEALING PHASE: During the healing phase the necrosis is reconstructed. Since the ciliary muscle is attached to the lens through the zonules, the Epileptoid Crisis manifests as a fluttering of the lens (compare with pupil spasms and nystagmus related to the extraocular muscles).
At the end of the healing phase, the ciliary muscle will be stronger than before. This principle, namely that an organ works more efficiently after healing has been complete, applies without exception to all cerebral medulla-controlled organs.
|
 DEVELOPMENT AND FUNCTION OF THE EXTRAOCULAR MUSCLES: The extraocular muscles are six small muscles that surround the eye and control its movement. Four rectus (“straight”) muscles regulate the movement of the eyeball from left to right and up and down: the superior rectus moves the eye upward, the inferior rectus moves the eye downward, the medial rectus moves the eye inward (towards the nose), and the lateral rectus moves the eye outward (away from the nose). The two oblique muscles are primarily responsible for rotating the eyes: the superior oblique rotates the eye inward and downward, the inferior oblique rotates the eye outward and upward. The extraocular muscles are mainly made of striated muscles originating from the new mesoderm. They are controlled from the cerebral medulla and the motor cortex (compare with smooth lateral rectus muscle).
BIOLOGICAL CONFLICT: The biological conflict linked to the extraocular muscles is “not wanting to look in a certain direction” because of something distressing “there”. Newborns, for example, suffer the conflict when they are blinded by bright fluorescent light in the delivery room. The extraocular muscles also correspond to “not being allowed to look there” (a student is caught cheating while he was trying to copy the exam from his neighbor) and “not being able to look there” (an infant is unable to look towards the mother).
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of muscle tissue (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing paralysis of the affected eye muscle (controlled from the motor cortex).
The paralysis or weakness of the eye muscle causes strabismus, the inability to attain binocular vision (see also strabismus caused by the damage of the oculomotor nerve due to a pineal gland tumor). Depending on the exact nature of the conflict, one or both eyes deviate inward, outward, upward or downward.
Strabismus esotropia (cross-eyed): one or both eyes deviate inward.
Strabismus exotropia (wall-eyed): one or both eyes deviate outward.
Strabismus hypertropia: one or both eyes deviate upward.
Strabismus hypotropia: one or both eyes deviate downward.
Cyclophoria is a type of strabismus in which the axis of one or both eyes rotates inward or outward due to the paralysis of the oblique muscles.
HEALING PHASE: During the healing phase the necrosis is reconstructed. The paralysis reaches into PCL-A. The Epileptoid Crisis presents as involuntary eye movement, called nystagmus. Depending on the exact nature of the conflict, the eyeball flutters up and down or side to side (compare with fluttering of the lens and pupil spasms). Recurring flutters are triggered by setting on a track that was established when the “don’t want to look there”-conflict took place. Uncontrollable eye movement could also occur together with a generalized seizure (grand mal) involving the entire motor cortex. After the Epileptoid Crisis, during PCL-B, the function of the eye muscle returns to normal.
At the end of the healing phase, the eye muscle will be stronger than before. This principle, namely that an organ works more efficiently after healing has been complete, applies without exception to all cerebral medulla-controlled organs.
Bulging eyes (proptosis, exophthalmos) is caused by an enlargement of structures within the eye socket pushing the globe of the eyes out of the orbit – like a telescope. Continuous swelling of the tear gland, for example, can lead to an anterior displacement of the eye. The same might occur with a buildup of connective tissue; in this case, the underlying conflict is a self-devaluation conflict. The condition, also known as Graves’ disease or Basedow disease, is generally associated with hyperthyroidism. From a GNM viewpoint, an overactive thyroid and a protrusion of the eyeball only occur together when the thyroid conflict is coupled with a self-devaluation conflict related to the eyes (“My eyes failed to be fast enough to catch or eliminate a morsel”).
In the event of an abandonment or existence conflict, the lateral rectus pulls the eye(s) outward. When the conflict impacts in the right kidney tubules relay, the right eye deviates towards the right; when the left kidney tubules are affected, the left eye deviates towards the left. With two active abandonment or existence conflicts involving both kidney tubules, both eyes deviate sideways (see KCT Constellation). This is commonly called a “lazy eye”, or amblyopia. It should not come as a surprise that the condition often occurs in children. If the smooth part of the lateral rectus is affected, the person is able to pull the eye voluntarily into the correct position since the eye muscle is not paralyzed. In this case, the person is conflict active with an abandonment or existence conflict rather than with a visual “stuck”-conflict related to the striated lateral rectus with paralysis in the conflict-active phase (see strabismus exotropia).
|








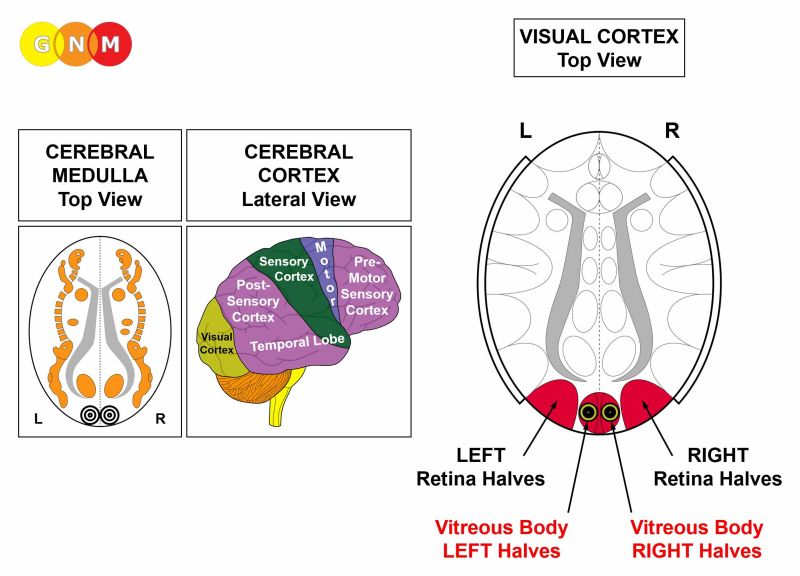
 DEVELOPMENT AND FUNCTION OF THE RETINA: The retina is a light-sensitive layer of nerves that lines the back of the eye. The retina contains neurons such as photoreceptors (rods and cones) that receive light and colors from the lens and convert them into impulses that are sent via the optic nerve to the visual cortex at the back of the brain. The macula, located near the central portion of the retina, is responsible for central vision. Within the central macula lies the fovea, which is a small pit that permits the highest visual acuity. The retina originates from the ectoderm and is controlled from the visual cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the retina relates to a fear that cannot be shaken off (compare with vitreous body), for example, the fear of losing a loved one or one's home, the fear of punishment, abuse, unemployment (debts, poverty), persecution (religious, ethnic, political), or the fear of having cancer (medical tests, follow-up examinations). Children suffer the conflict when they witness domestic violence.
CONFLICT-ACTIVE PHASE: functional loss due to the loss of retinal photoreceptor cells with the biological purpose to make that what evokes the fear temporarily invisible (when children are scared, they cover their eyes). The loss of rod cells, responsible for vision at low light levels, results in nyctalopia or “night blindness” with difficulties seeing in dim light or in the dark.
Intense conflict activity leads to a diminished vision in a defined area of the visual field (scotoma) as a result of the breakdown of retinal cells (compare with scintillating scotoma). However, with a moderate conflict, the reduced vision might not be noticed since the other retina halves compensate the vision loss.
HEALING PHASE: During the healing phase the function of the photoreceptor cells is restored. In PCL-A an edema forms between the choroid and the affected area of the retina. During the Epileptoid Crisis the edema is expelled, which is noticeable as flashes of light (photopsia). The flashes could be short bursts or happen continually until the retina is repaired.
Recurring conflict relapses lead to the buildup of scar tissue and a hardening (callosity) in the retina. If the hardening occurs laterally (on the side), the eyeball elongates causing nearsightedness or myopia (see also smooth ciliary muscle and cornea), whereas hardening in the back (dorsal) compresses the eyeball causing farsightedness or hyperopia (see also lens and striated ciliary muscle in both eyes). At this point the condition is irreversible.
A large edema between the choroid and retinal layer (usually because of water retention due to the SYNDROME) pulls the retina from its normal position. This is generally called a retinal detachment (strictly speaking, a misnomer since the retina does not “detach”). With no conflict relapses the condition reverses on its own. However, if the fear-conflict persists healing cannot be complete and the vision becomes drastically reduced. The panic of becoming blind often adds new fears creating a progressive condition. CAUTION: Stooping or physical exertion, for example when lifting something heavy, can cause a rupture of the retina!
What is termed “diabetic retinopathy” is based on the assumption that an elevated blood sugar level damages the retina. Yet, not every diabetic develops the condition! From the GNM point of view, it is the additional resistance conflict (a resistance to the fear-provoking situation) why the two Biological Special Programs often run simultaneously (see also “diabetic peripheral neuropathy” related to the periosteum).
|









 DEVELOPMENT AND FUNCTION OF THE VITREOUS BODY: The vitreous body occupies the space between the lens and the retina at the back of the eye. Fluid produced in the ciliary body fills the vitreous with a gel-like substance made up of about 99% water. The gel, composed mainly of collagen, is transparent so that light rays are able to pass through it to reach the retina. The intraocular pressure maintains the shape of the eye and prevents the walls of the eyeball from collapsing. The sclera, a sheath of connective tissue, supports the eyeball from the outside. The vitreous body consists of mesodermal parts, controlled from the cerebral medulla, and ectodermal parts, controlled from the visual cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the vitreous body is a fear of a “predator” who is “sneaking up from behind” (compare with a “fear that cannot be shaken off” related to the retina). Thus, the conflict is always a fear of a person, for example, the fear of an abuser, a stalker, a character assassin, a threatening ex-spouse, a relative who is after one’s inheritance, a supervisor, a teacher, a parent, a doctor, a lawyer, or an authority (government, tax office, bailiff, police, judge) that is “breathing down one’s neck”. The fear could also be experienced as feeling pressured by someone to perform(at school, at home, at work).
CONFLICT-ACTIVE PHASE: necrosis (controlled from the cerebral medulla) and functional loss of the vitreous body (controlled from the visual cortex), causing an interference of the transmission of light to the retina and consequently a clouding of the vitreous (compare with clouding of the lens). Considering that due to the refraction of light by the cornea and the lens the images projected onto the retina are reversed (what is perceived in the temporal field of vision is registered on the nasal vitreous), the clouding of the vitreous affects predominantly the nasal halves and therefore the peripheral vision (see visual fields). The biological purpose of the clouding is to blur the sight of the “predator” (horse-blinkers phenomenon) to be able to focus fully on the escape route.
HEALING PHASE: During the healing phase the clouding of the vitreous body recedes. In PCL-A an edema (fluid accumulation) develops at the site, which increases the intraocular pressure in the eye. With the SYNDROME, that is, with water retention as a result of an active abandonment or existence conflict, the eye pressure rises even more. During the Epileptoid Crisis the edema is pressed out. However, in order to keep the eyeball firm and prevent it from collapsing, the intraocular pressure remains elevated during and shortly after the Epileptoid Crisis (in PCL-B). With a hanging healing due to continuous conflict relapses the optic nerve becomes damaged, particularly when the edema reaches into the opening of the vitreous where the optic nerve leaves the eye. In conventional medicine, damage to the optic nerve is called a glaucoma or “green cataract” (compare with “grey cataract” related to the lens).
The scarring process (PCL-B) in the vitreous body is noticeable as eye floaters (mouches volantes) that appear as spots, threads, black or grey specks, strings or cobwebs that drift about with the movement of the eyes. Floaters are visible because of the shadows they cast on the retina. After the healing process has been completed, the floaters disappear. With a hanging healing the vitreous body slowly shrinks and pulls away from the retina. This is called a vitreous detachment. What is known as a “Weiss ring” is a circle-shaped floater that is created by a posterior vitreous detachment around the optic nerve in the back of the eye (compare with retinal detachment). The separation from the retina causes damage to the retina’s surface. When this occurs, the retina initiates a healing process and forms scar tissue, or an epiretinal membrane. If the scar tissue forms over the macula, the part of the eye responsible for central vision, this is called a macular pucker, as it causes the macula to “pucker” or wrinkle as it shrinks (compare with macular degeneration).
|






{kind=link}
{kind=link}
{kind=link}