
INTESTINES and RECTUM
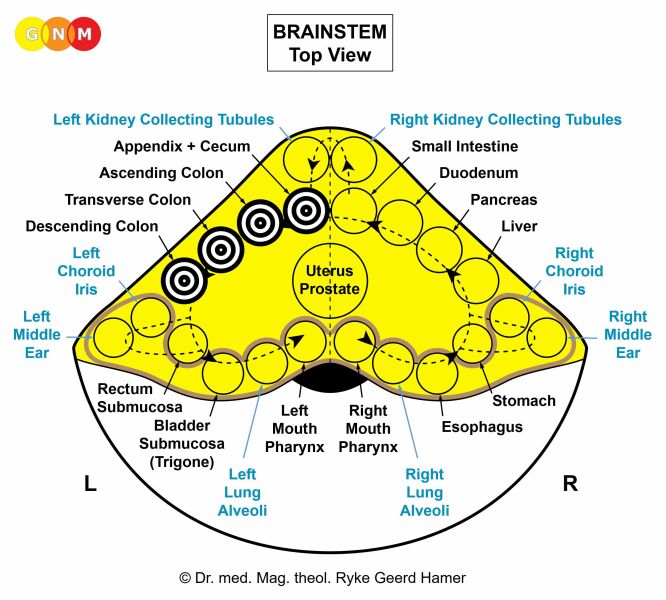
 DEVELOPMENT AND FUNCTION OF THE SMALL INTESTINE: The small intestine is the portion of the gastrointestinal tract that connects the stomach with the colon. Following the duodenum, the jejunum is the upper part of the small intestine; the ileum is the final part that joins with the large intestine. The jejunum and ileum are the sections of the digestive tract where most of the absorption of nutrients (absorptive quality) takes place. The small intestine consists of intestinal cylinder epithelium, originates from the endoderm and is therefore controlled from the brainstem.
BIOLOGICAL CONFLICT: According to its function, the biological conflict linked to the small intestine is “not being able to absorb or digest a morsel” (see also stomach, duodenum, colon, and pancreas gland). The conflict is experienced as anger, for instance, anger about a person (a family member, friend, neighbor, colleague, employee, supervisor, client, teacher, student, classmate, coach, doctor, authorities), about a situation (work-related anger, school-related anger, relationship-related anger), or about remarks (accusations, insults, criticism) or news that are “hard to take” or difficult to “digest”.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase intestinal cells proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to be better able to absorb and digest the morsel. With prolonged conflict activity a flat growth (absorptive type) develops in the small intestine. At the distal end of the ileum, which has a thinner wall than the jejunum, the growth can also take a cauliflower-shaped form (secretory type). This could lead to a bowel obstruction or so called ileus. In conventional medicine, the thickening of the intestinal wall might be diagnosed as a cancer (jejunal cancer or ileal cancer).
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. Healing symptoms are diarrhea and vomiting if the jejunum (upper part of the small intestine) is involved, and night sweats. Abdominal cramps (motor quality) occur particularly during the Epileptoid Crisis (see also intestinal colic). The participation of fungi during the healing process manifests as intestinal candidiasis. The extent of the symptoms is determined by the degree of the conflict-active phase.
Crohn’s Disease is the healing phase of an “indigestible morsel conflict”. Ileocolitis, affecting the final section of the small intestine, is the most common type of Crohn’s. Symptoms are persistent diarrhea with the elimination of mucus, usually with blood (tarry stool), abdominal pain, and an inflammation of the bowel. A chronic condition indicates that conflict relapses prolong the healing process (hanging healing). Characteristic for recurring Crohn’s are flare-ups that occur every time the person sets on a track with condition-free periods in between.
Food allergies with recurring diarrhea reveal that an “indigestible anger” related to a particular food (milk, nuts, wheat, seafood, a certain fruit or vegetable) has not been completely resolved. Multiple food allergies indicate that several foods, including food elements (sugar, salt, lactose), are stored in the subconscious as tracks linked to the original DHS. Any food that is believed to be the probable source of the “allergy” constitutes a new “indigestible morsel” and is added to the list of conflict tracks. People who are always concerned about eating something “toxic” or “wrong” are therefore more prone to develop multiple food allergies. In the case of “gluten intolerance”, or celiac disease, gluten, found in wheat and related grains, is associated with an “indigestible anger conflict”. The repetitive contact with the wheat (“allergen”) leads eventually to an inflammation in the small intestine. A gluten-free diet, the standard recommended treatment, translates into staying away from the gluten-track without addressing the real cause.
| ||||||||||


 DEVELOPMENT AND FUNCTION OF THE COLON: Following the small intestine, the colon is the last portion of the gastrointestinal tract. The colon is divided into several structural parts. The first section of the large intestine is the cecum with the appendix, a pouch-like blind-ended tube attached to the ascending colon. The transverse colon extends from the right to the left side of the body, where it joins the descending colon. The sigmoid colon is the final section of the large intestine. Originally the entire intestinal canal served the absorption (absorptive quality) and digestion (secretory quality) of food. Today, the colon only secretes mucus and is the part of the intestinal tract where waste material from food is processed into feces and carried to the rectum, from where it is eliminated. The colon consists of intestinal cylinder epithelium, originates from the endoderm and is therefore controlled from the brainstem.
BIOLOGICAL CONFLICT: The biological conflict linked to the colon (except the sigmoid colon) is an “indigestible morsel conflict” (see also stomach, duodenum, small intestine, and pancreas gland). For animals an indigestible morsel is a real piece of food; for humans, it can also be a figurative “morsel”, for example, a car, a house, or a valuable object. We might also perceive certain circumstances or an unpleasant event as a “morsel” and suffer the conflict when the situation is considered as “indigestible” or “non-absorbable”, let’s say, when an anticipated purchase, promotion, or promise cannot be “taken in”. The distinctive aspect of the morsel conflict corresponding to the colon, including the appendix and the cecum, is that the conflict is experienced as particularly “ugly”, for instance, ugly fights over money or over a property, ugly divorces, ugly court cases, or ugly betrayals.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the large intestine proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to facilitate the digestion of the morsel. Even though the colon has no longer a digestive function, in the event of a biological conflict, the large intestine still responds with cell augmentation because originally the entire intestinal canal served the digestion of food. With prolonged conflict activity (hanging conflict) a tumor or colon cancer develops as a result of the continuing cell augmentation. The tumor grows either on a flat plane (absorptive type) or takes a cauliflower-shaped form (secretory type). If the rate of cell division exceeds a certain limit, conventional medicine considers the cancer as “malignant”; below that limit, the growth is regarded as “benign” or diagnosed as an intestinal polyp (see also healing phase). There are no symptoms during the conflict-active phase. However, a large tumor causes a narrowing of the colon (with “pencil stool”), which might lead to an obstruction of the bowel requiring surgery.
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. Healing symptoms are diarrhea (excretory quality), blood in the stool (tarry bowel movements), abdominal cramps (motor quality), particularly during the Epileptoid Crisis (see intestinal colic), and night sweats. An “intestinal yeast overgrowth” indicates that fungi assist the healing process. An “intestinal infection” with (bloody) diarrhea and abdominal pain can also be caused by the participation of Escherichia coli (E. coli) bacteria that colonize the small and large intestines (see E.coli infection in the endodermal bladder trigone). Depending on the degree of the conflict-active phase, the symptoms range from mild to severe.
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells remain. Eventually, the growth becomes encapsulated. In conventional medicine, this is most likely diagnosed as an intestinal polyp or a “benign cancer” (see also conflict-active phase).
With the SYNDROME due to an active abandonment or existence conflict involving the kidney collecting tubules the retained water is exceedingly stored in the healing area. The enlarged swelling could obstruct the colon; in the appendix, an occlusion might already occur during the conflict-active phase. It is during the healing phase that the appendix becomes inflamed causing appendicitis. A rupture of the appendix happens when the Epileptoid Crisis is intense.
Colitis is an inflammation of the bowel with abdominal pain, flatulence, and diarrhea, potentially with blood in the stool. Like Crohn’s Disease, colitis ulcerosa develops after the conflict resolution (CL). Persistent symptoms point to conflict relapses that interrupt and therefore prolong healing (hanging healing). What is known as “Irritable Bowel Syndrome” (IBS) is also a sign that an “indigestible morsel conflict” has been resolved. Compared with colitis, the symptoms are less intense.
Diverticulitis is the result of extended healing in the intestine. Because of the continuous cell removal process, the intestinal wall becomes thin leading to the formation of pouches (diverticula) on the outside of the colon. Diverticulitis is the condition when such a pouch becomes inflamed due to conflict relapses.
|

 DEVELOPMENT AND FUNCTION OF THE INTESTINAL MUSCLES: The wall of the small intestine and the colon consists of smooth muscles. The longitudinal muscles regulate the muscle contraction while the transverse muscles regulate their relaxation. The alternating rhythm of contraction and relaxation causes the peristaltic motion (motor quality) that moves the “food morsel” along the intestinal canal (see also heart muscle/“blood morsel”; pupil muscles/“light morsel”). The smooth muscles of the intestine originate from the endoderm and are controlled from the midbrain.
BIOLOGICAL CONFLICT: The biological conflict linked to the intestinal muscles is “not being able to pass an indigestible morsel”. This relates to a “morsel” in real terms (a piece of food) or figurative terms (something “indigestible” is not “moving forward”, for example, a court case).
CONFLICT-ACTIVE PHASE: increased local tonic muscle contraction (hypertonus). The local peristalsis (local colic) serves the biological purpose to push the morsel further with greater force. During this period, the peristalsis in the other parts of the intestine slows down causing constipation and abdominal bloating due to the expansion of the intestinal muscles. NOTE: Constipation can occur during any given conflict-active phase, since in sympathicotonia digestion slows down; the same happens with too little fluid intake (see also decreased urine output, linked to the kidney collecting tubules, causing dry and hard stool that is difficult to pass).
HEALING PHASE: clonic hyperperistalsis of the entire intestine (intestinal colic); during the Epileptoid Crisis strongly increased local tonic cramps and flatulence (stagnant peristalsis in the remaining intestine). NOTE: When striated muscles, for example of the skeletal muscles, go through the Epileptoid Crisis, the tonic and clonic cramps occur together. – If the abdominal cramps (motor quality) are followed by diarrhea (sensory quality) this indicates that the Biological Special Programs of the intestinal mucosa and intestinal muscles run concurrently (digesting and passing the “indigestible morsel”).
|

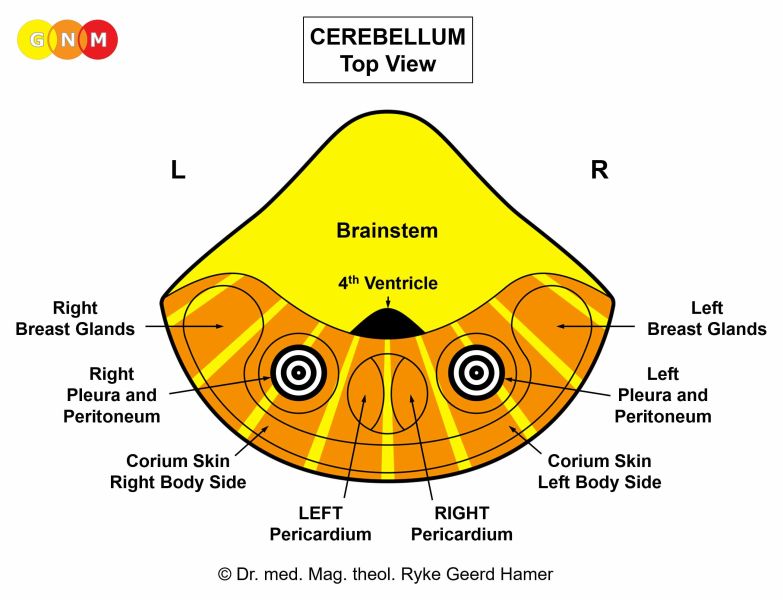
 DEVELOPMENT AND FUNCTION OF THE PERITONEUM: The peritoneum consists of a two-layered serous membrane. The parietal peritoneum lines the abdominal cavity whereas the visceral peritoneum (including the retroperitoneum) covers the individual organs such as the liver, spleen, pancreas, stomach, duodenum, small intestine, colon with the omentum, the upper part of the rectum, kidneys, bladder as well as the uterus, ovaries, and testicles (tunica vaginalis testis). The peritoneal cavity between the two peritoneal layers is filled with fluid that lubricates the peritoneal surfaces. In evolutionary terms, the peritoneum developed together with the pleura, the pericardium, and the corium skin. The peritoneum originates from the old mesoderm and is therefore controlled from the cerebellum.
BIOLOGICAL CONFLICT: The biological conflict linked to the peritoneum is an attack conflict, specifically, an attack against the abdomen (see also attack conflicts related to the pleura, pericardium, and corium skin).
An attack against the abdomen is experienced, for instance, through an attack by an animal or through a kick, punch, or stab into the stomach or belly during a fight; the same applies to attacks from behind against the kidneys. “Sharp” words or threats (“I’ll kill you!”) directed at someone can also be registered as an attack, affecting the retroperitoneal space if the verbal insult is perceived as a “stab in the back”. However, surgery in the abdominal area (cesarean, hysterectomy, removal of a tumor, kidney or liver transplant), the fear of an operation (picturing “being cut open”), invasive wound pumps, peritoneal dialysis tubing (insertion of a catheter in the abdominal wall to filter the blood), or biopsies and punctures of the abdomen, including amniotic fluid tests where the uterus, the sac that surrounds the fetus, is punctured, also trigger the conflict. The diagnosis of a colon cancer, ovarian cancer, or liver cirrhosis can be perceived as an “attack” concerning the integrity of the organ. Attack conflicts also originate from inside, for instance, through acute abdominal pain (stomach ache, intestinal colic, menstrual pain) or pain during intercourse.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase peritoneal cells proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to create an internal reinforcement to protect the abdomen against further attacks. With prolonged conflict activity (hanging conflict) a bulb-shaped growth forms at the site; cell augmentation on a flat plane usually occurs when the attack conflict was more of a general nature. In conventional medicine, the thickening of the peritoneum is diagnosed as a (retro)peritoneal mesothelioma (see also omental mesothelioma, pleural mesothelioma, pericardial mesothelioma, and testicular mesothelioma). If the rate of cell division exceeds a certain limit, then the cancer is considered “malignant”.
HEALING PHASE: Following the conflict resolution (CL), fungi, TB bacteria or other bacteria remove the cells that are no longer needed. Healing symptoms are abdominal pain and night sweats. With an inflammation the condition is called peritonitis. After the additional cells have been decomposed, caverns remain at the site. Over time, these caverns are filled with calcium showing on an X-ray as calcium deposits.
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells remain. Eventually, the growth becomes encapsulated with connective tissue. Now, conventional medicine regards the cancer as “benign”.
During the healing phase (in PCL-A) the fluid in the peritoneum is naturally absorbed by the peritoneal membrane (dry peritonitis). Water retention, however, due to the SYNDROME increases the accumulation of fluid (wet peritonitis) causing acute pain. If bacteria assist healing, the fluid contains pus (purulent peritonitis, tuberculous peritonitis). Since the peritoneum is not divided into a right and left part, the exudative peritoneal effusion (buildup of excessive fluid) develops in the entire peritoneum (compare with pleural effusion and pericardial effusion). Only the location of the Hamer Focus in the brain reveals on which side of the abdomen the attack was perceived and therefore from which brain hemisphere the Biological Special Program is directed and controlled.
Concurrent water retention as a result of an active abandonment or existence conflict presents as an abdominal ascites. If a person is overweight the ascites might not be noticed.
In people with liver cirrhosis, standard medicine attributes the fluid accumulation in the peritoneum to high blood pressure in the portal vein of the liver. From a GNM point of view, the ascites rather reveals recurring territorial anger conflicts affecting the bile ducts and ongoing abandonment or existence conflicts.
Peritoneal fluid is rich in protein. Thus, draining the excess fluid could lead to serious complications since the body tries to replenish the protein shortage by withdrawing it from the organs, which causes rapid weight loss. According to Dr. Hamer, 60-70% of patients die from such complications. He, therefore, advises not to drain more than 1.5 liters at a time in order to prevent an acute protein deficiency. Moreover, puncturing the peritoneum triggers often new attack conflicts and conflict relapses with each procedure, throwing the person into a vicious cycle. Dr. Hamer recommends staying away from a puncture all together and to use instead a small balloon catheter that allows patients to regulate the drainage of the ascites themselves.
The GREAT OMENTUM (epiploon) is a double peritoneal fold that hangs like an apron over the intestine giving the abdomen further protection. The lubricated surface of the membrane (secretory quality) provides the omentum with a special motility.
BIOLOGICAL CONFLICT: The biological conflict linked to the great omentum is an ugly belly conflict, experienced as acute distress in relation to the abdomen. Liver cirrhosis, a colon cancer or ovarian cancer diagnosis could evoke the conflict.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the omentum proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to enhance the secretion of lubricating fluid to improve the motility of the omentum. This also allows to envelop inflammatory sites (cold abscesses) or to seal a perforated appendix, preventing intestinal content from leaking into the abdomen. With ongoing conflict activity (hanging conflict) a cauliflower-shaped growth (secretory type) forms as a result of the continuing cell augmentation. In conventional medicine, this is diagnosed as an omental mesothelioma (see also peritoneal mesothelioma, pleural mesothelioma, pericardial mesothelioma, and testicular mesothelioma). If the rate of cell division exceeds a certain limit, then the cancer is considered “malignant”.
HEALING PHASE: Following the conflict resolution (CL), fungi, TB bacteria or other bacteria remove the cells that are no longer needed. Adhesions occur as a result of a prolonged healing process (hanging healing).
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells remain. Eventually, the growth becomes encapsulated with connective tissue. In this case, the “cancer” is interpreted as “benign”.
|


RECTUM
 DEVELOPMENT AND FUNCTION OF THE SIGMOID COLON AND RECTUM SUBMUCOSA: The sigmoid colon is the final portion of the large intestine joining the rectum. The rectum connects with the anus, the opening where waste matter in form of stool passes out of the body. To facilitate the expulsion of fecal matter, the rectal sphincters relax to allow feces to exit the intestinal canal. The sigmoid colon and rectal submucosa consist of intestinal cylinder epithelium, originate from the endoderm and are therefore controlled from the brainstem.
BIOLOGICAL CONFLICT: The biological conflict linked to the sigmoid colon and rectum submucosa is a “feces conflict”, or “shit conflict”. The conflict is either about a real “feces”-morsel (human feces or animal poo) or is experienced in a figurative sense triggered, for example, by dirty business, malicious slander, mean accusations, in short, by a “shitty” incident (compare with feces conflict related to the perianal ducts and the sigmoid/rectal muscles).
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the sigmoid colon and/or rectum proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to facilitate the digestion of the morsel. Even though the rectum has no longer a digestive function, in the event of a biological conflict, the organ still responds with cell augmentation because originally the entire intestinal canal served the digestion of food. With prolonged conflict activity (hanging conflict) a flat (absorptive type) or cauliflower-shaped growth (secretory type) develops in the sigmoid (immediately above the rectum) or in the rectum (underneath the rectum surface mucosa). In conventional medicine, this is diagnosed as a colorectal cancer (compare with “rectal cancer” related to the rectum surface mucosa). If the rate of cell division exceeds a certain limit, the cancer is considered as “malignant”; below that limit, the growth is regarded as “benign” or diagnosed as a rectal polyp (see also healing phase).
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. Healing symptoms are rectal bleeding, tarry bowel movements, and night sweats. Rectal cramps or spasms (motor quality) occur during the Epileptoid Crisis (see also rectal spasms related to the rectum surface mucosa, smooth rectal muscles, internal rectal sphincter, and striated rectal muscles and external rectal sphincter). Depending on the degree of the conflict-active phase, the symptoms range from mild to severe.
Like colon cancers, rectal cancers are usually only found in the healing phase when they start to bleed and cause discomfort. With water retention due to the SYNDROME the swelling enlarges and might cause a rectal obstruction (in PCL-A). After the Epileptoid Crisis the swelling recedes.
When TB bacteria remove a tumor in the rectum, an abscess might form in the course of the healing process. In conventional medicine, such rectal abscesses with swelling and discharge of blood are often misdiagnosed as hemorrhoids.
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells in the rectum remain. Eventually, the growth becomes encapsulated. In conventional medicine, this is usually diagnosed as a “benign cancer”, a rectal polyp (see also conflict-active phase), or as hemorrhoids.
|

 DEVELOPMENT AND FUNCTION OF THE RECTUM SURFACE MUCOSA: The rectal surface mucosa covers about 12 cm of the endodermal submucosa in the lower section of the rectum. The surface mucosa consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex. The inner wall of the lower rectum is endowed with striated muscles.
BIOLOGICAL CONFLICT: The biological conflict linked to the rectal surface mucosa is a female identity conflict or male territorial anger conflict, depending on a person’s gender, laterality, and hormone status (see also Aggressive Constellation).
An identity conflict refers to the inability to establish one’s position or place (“territory”), literally or figuratively. An unwanted move, change of school, or change of a workplace can activate the conflict. Feeling unsettled, not knowing where to belong, not finding one’s place in a relationship, within the family, the group at work, or in the culture and society at large as well as discrimination against one’s belief or sexual orientation are examples of what can evoke an identity conflict. The conflict is to a certain extent a decision conflict (not knowing what choice to make, not knowing where to go).
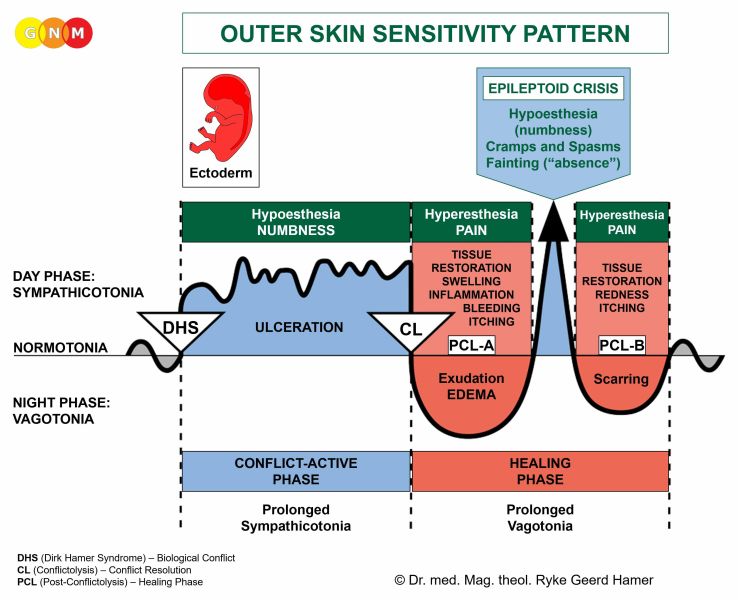
CONFLICT-ACTIVE PHASE: ulceration in the epithelial lining of the rectum proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the rectum to allow faster defecation in order to be better able to establish one’s place.
With prolonged conflict activity the continuing tissue loss in the rectum lining causes small tears or so called anal fissures. An anal fissure can burst open, for example, with the passing of hard stool.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation. Proctitis occurs when the healing process in the rectal lining is accompanied by an inflammation. The swelling, caused by the edema, presents as hemorrhoids in the lower rectum (internal hemorrhoids) or around the anus (external hemorrhoids). With water retention due to an active abandonment or existence conflict (the SYNDROME) hemorrhoids become much larger. In conventional medicine, the “growth” might be diagnosed as a “rectal cancer” (compare with rectal cancer related to the rectum submucosa). Based on the Five Biological Laws, the new cells cannot be regarded as “cancer cells” since the cell increase is, in reality, a replenishing process.
Healing symptoms are burning pain in the rectum, anal itching, rectal bleeding (with hard bowel movements hemorrhoids crack and bleed), and painful rectal muscle cramps or spasms if the surrounding striated muscles of the inner rectum wall undergo the Epileptoid Crisis at the same time (see also rectal spasms related to the rectum submucosa, smooth rectal muscles, internal rectal sphincter, or striated rectal muscles and external rectal sphincter). Depending on the intensity of the conflict-active phase, the symptoms range from mild to severe. Typical for the healing phase is the feeling of incomplete emptying of the bowels following defecation, termed rectal tenesmus (compare with bladder tenesmus).
Conventional medicine claims that hemorrhoids are “varicose veins” in the rectal area. In reality, the swelling occurs in the epithelial mucosa of the rectum. Dr. Hamer's brain scan studies demonstrate that every person who has hemorrhoids shows the Hamer Focus in the cerebral cortex in the control center of the rectum surface mucosa and not in the cerebral medulla from where the blood vessels are controlled (see also esophageal varices, erroneously linked to liver cirrhosis).
According to statistics, hemorrhoids are more common in women during pregnancy. They are said to be caused by the weight carrying the baby. From the GNM perspective, a pregnant woman only develops hemorrhoids, when she is in the healing phase of an identity or decision conflict. This is why not every pregnant woman has the condition.
Surgical removal of hemorrhoids is only a temporary “solution” because, if the conflict has not been completely resolved new hemorrhoids start developing with the next conflict relapse, triggered by setting on a track that was established when the original identity conflict took place.
|
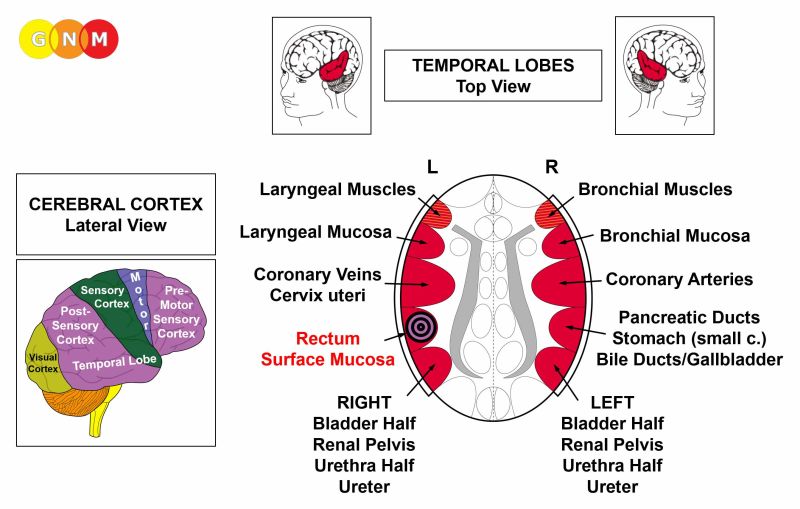



 DEVELOPMENT AND FUNCTION OF THE PERIANAL DUCTS: The perianal ducts carry fluid produced in the anal glands into the rectum to aid defecation. The glands themselves are located on either side of the anus between the internal and external rectal sphincter. In mammals, these glands are referred to as “scent glands” because they enable the animals to mark their territory (in addition to feces and urine) and to identify members within a species. The lining of the perianal ducts consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the perianal ducts is “not being able to eliminate feces fast enough”. Such a “feces conflict” can be experienced in real terms (constipation) or in a transposed sense triggered, for example, by a “shitty” situation one is unable to “evacuate” fast enough (compare with feces conflict related to the sigmoid/rectum submucosa and sigmoid/rectal muscles).
CONFLICT-ACTIVE PHASE: ulceration in the lining of the perianal ducts proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the lumen to facilitate faster defecation.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation. The edema (fluid accumulation) creates a perianal cyst. If there are no conflict relapses, the cyst recedes during the healing phase. A perianal abscess develops when bacteria assist the healing process.
With a hanging healing, a chronic perianal abscess or the continuous pressure of a cyst might form a perianal fistula, an opening (tunnel) between the anal canal and the skin near the anus (see also thyroid fistula). This usually occurs when large amounts of water are retained in the cyst due to the SYNDROME or as a result of conflict relapses that prolong the healing process.
|

 DEVELOPMENT AND FUNCTION OF THE SIGMOID AND RECTAL MUSCLES (UPPER RECTUM): Like the intestines, the sigmoid colon and upper part of the rectum consist of smooth muscles originating from the endoderm and controlled from the midbrain.
BIOLOGICAL CONFLICT: The smooth muscles of the sigmoid and upper part of the rectum are linked to a “feces conflict”, or “shit conflict”, experienced in real terms (fecal incontinence, persistent constipation) or in a transposed sense, as a “shitty” situation (see also feces conflict related to the sigmoid colon and rectum submucosa and the perianal ducts).
CONFLICT-ACTIVE PHASE: increased muscle tension (hypertonus)
HEALING PHASE: muscle relaxation with rectal spasms during the Epileptoid Crisis (see also rectal spasms related to the internal rectal sphincter, striated rectal muscles and external rectal sphincter, rectum submucosa, and rectum surface mucosa).
Rectal prolapse: The rectum is attached to the pelvis by muscles and ligaments that hold the rectum in place. A lasting self-devaluation conflict (chronic constipation, chronic diarrhea, long-term hemorrhoids) progressively weakens the pelvic floor muscles causing the rectum to protrude out of the anus (compare with uterine prolapse). In infants, a rectal prolapse might be related to distressing potty training triggered, for example, because of scolding, punishments, or failing expectations of a parent. A weakness of the anal sphincter (external rectal sphincter) could also lead to a rectal prolapse. In this case, the condition concurs with fecal incontinence, a leakage of stool.
|
 DEVELOPMENT AND FUNCTION OF THE INTERNAL RECTAL SPHINCTER: The internal and external rectal sphincters control the closing of the anus and the elimination of feces. The internal rectal sphincter is a muscular ring that surrounds the anal canal. It is formed by a thickening of the circular muscles of the rectum. The internal rectal sphincter consists of smooth muscles, originates from the endoderm, and is controlled from the midbrain.
BIOLOGICAL CONFLICT: The biological conflict linked to internal rectal sphincter is not being able to hold back feces, for example, because of fecal incontinence.
CONFLICT-ACTIVE PHASE: hypertonus of the internal rectal sphincter. The biological purpose of the increased muscle tension is to facilitate holding back the feces.
HEALING PHASE: The muscle tension goes back to normal. The Epileptoid Crisis presents as painful rectal spasms (see also rectal spasms related to the smooth rectal muscles, striated rectal muscles and external rectal sphincter,rectum submucosa, and rectum surface mucosa).
|
 DEVELOPMENT AND FUNCTION OF THE RECTAL MUSCLES (LOWER RECTUM) AND EXTERNAL RECTAL SPHINCTER: The external rectal sphincter is a muscle that surrounds the anus immediately beneath the skin. Like the internal rectal sphincter, it regulates the closing and opening of the anus in order to hold and expel feces. The lower part of the rectal muscles and the external rectal sphincter consist of striated muscles, originate from the new mesoderm and are controlled from the cerebral medulla and the motor cortex.
BIOLOGICAL CONFLICT: The biological conflict linked to the rectal muscles and external rectal sphincter is the same as with the rectum surface mucosa, namely, an identity conflict in the sense of an inability to establish one’s position or place. Biologically, this translates into “not being able to sufficiently mark one’s territory” (by defecation), similar to the marking conflict related to the bladder muscle and external bladder sphincter.
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of rectal muscle tissue (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing paralysis of the rectal muscles (controlled from the motor cortex). At the same time, the rectal sphincter opens (no necrosis with sphincters!) which allows to better mark one’s place.
Persistent conflict activity causes fecal incontinence, an inability to control bowel movements (see also urinary incontinence). A sudden leakage of stool flow also occurs during the Epileptoid Crisis when the rectal sphincter opens.
HEALING PHASE: During the healing phase, the rectal muscles are reconstructed and the rectal sphincter closes. The Epileptoid Crisis manifests as painful rectal spasms (see also rectal spasms related to the internal rectal sphincter, smooth rectal muscles, rectum submucosa, and rectum surface mucosa).
| |||||||||||||||||||




{kind=link}
{kind=link}
{kind=link}
{kind=link}