DEVELOPMENT AND FUNCTION OF THE NASAL MUCOSA: The nasal cavity is divided into a right and left passageway that connect with the paranasal sinuses through small orifices. In the back they join with the nasopharynx and the mouth. Of the five senses (sight, smell, taste, touch, hearing) the olfactory sense is the oldest. In humans, it is the most powerful sense at birth. The sense of smell is to a large extent linked with the sense of taste. The mucosa covering the inside of the nose cleans and moistens the air before entering the lungs. The nasal mucosa consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
NOTE: The nasal cavities are no longer endowed with an endodermal submucosa. However, the epithelial nasal mucosa still contains residues of endodermal cells (“nasal glands”) that produce nasal mucus (see also paranasal sinuses).
|
|
|
BRAIN LEVEL: The nasal mucosa is controlled from the sensory cortex (part of the cerebral cortex). The mucosa of the right nasal cavity is controlled from the left side of the sensory cortex; the mucosa of the left nasal cavity is controlled from the right cortical hemisphere (deep basal). Hence, there is a cross-over correlation from the brain to the organ (see GNM diagram showing the sensory homunculus).
|
BIOLOGICAL CONFLICT: The biological conflict linked to the nasal mucosa is according to its function a scent conflict (see also paranasal sinuses and “scent morsel” conflict related to the nasopharynx). For animals, the conflict might be provoked by the scent of an approaching predator or the smell of poisonous fumes. For humans, the conflict translates into “smelling” trouble or a potential threat, for instance, “smelling” a competitor or an opponent at work, at school, at home, or in a relationship. The nasal mucosa corresponds also to a stink conflict. A stink conflict is experienced in real terms through an offending odor or unpleasant smell, but also if the particular smell is associated with danger. The exposure to cigarette smoke can, therefore, trigger the conflict for someone who believes that second-hand smoke causes lung cancer. In a transposed sense, a stink conflict relates to any situation that is perceived as “This stinks!” or “I am fed up with this!”. This might also concern an annoying person (a “pest”). It is a type of “ separation conflict”.
NOTE: Whether the right or left nasal cavity is affected is determined by a person’s handedness and whether the conflict is mother/child or partner-related. A general “stink conflict” affects both sides.
|
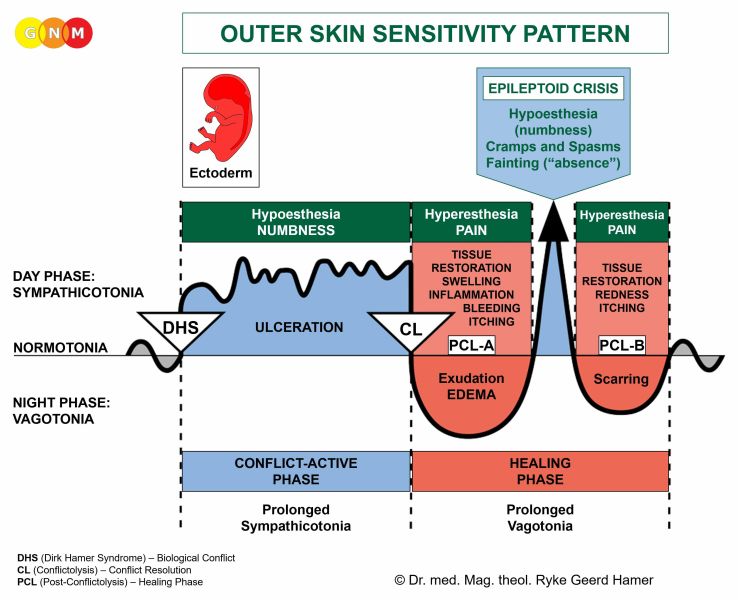
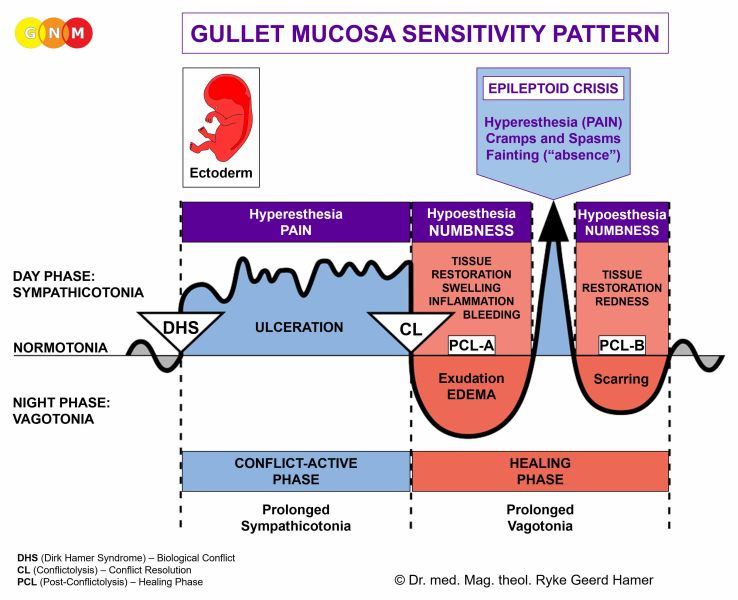
CONFLICT-ACTIVE PHASE: ulceration of the nasal mucosa proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the nasal passages in order to enhance the sense of smell (in Nature, smelling a predator or other potential dangers is essential for survival). Symptom: a dry nose due to the loss of nasal mucus-producing cells. During the conflict-active phase, the ulcers don't bleed. However, with a hanging conflict, they form crusts.
HEALING PHASE: During the first part of the healing phase (PCL-A) the ulcerated area is replenished through cell proliferation. Healing symptoms are a stuffed up nose caused by the swelling of the nasal membrane, a reduced sense of taste and smell (compare with anosmia related to the olfactory nerves), nasal discharge to eliminate the remnants of the repair process, headaches because of the brain edema in the corresponding brain relay, elevated temperature or fever, and fatigue since the autonomic nervous system is in the “warm phase” and in a prolonged state of rest (vagotonia). The shivers occur in the conflict-active “cold phase” as well as throughout the Epileptoid Crisis. Sneezing and nosebleeds are also a sign of the Epi-Crisis. In short, the healing phase of the nasal mucosa presents as the typical common cold. The degree of the symptoms is determined by the intensity of the conflict-active phase.
If a number of people have a cold at the same time, we can conclude that everyone who is affected had perceived a certain conflict situation the same way (troubles in daycare or kindergarten, poor marks for all students, an unfair teacher, arguments involving several family members, problems at the workplace) and is now in healing. In the northern hemisphere such collective “This stinks!”-conflicts are usually brought on at the beginning of the winter season – but only for those who “ hate winter”. In spring, the same symptoms are referred to as the “seasonal flu”.
Conventional medicine claims that the cold or flu (see also influenza) are caused by viruses. However, to this day, the evidence of the existence of these alleged viruses has never been provided (details presented in the “Virus Mania” GNM video). Moreover, the symptoms of the cold and flu are healing symptoms, which highly questions the persistent claim that they are “contagious”. Recurring or chronic cold symptoms occur when the scent or stink conflict is reactivated by setting on a conflict track such as a certain smell (food, perfume, flower, grass, cigarette smoke) or taste (milk, nuts, a spice), pet dander, pollen, mold, wind, rain, and so forth. In conventional medicine, this is usually interpreted as an “allergy”. People with pollen allergies might, in reality, be “allergic” to the cold symptoms (“This stinks!”) or to the “threat” of the “allergy season” resulting in common-cold symptoms (termed “allergic rhinitis”) each year. If the nasal congestion is accompanied by watery eyes (see conjunctivitis) then the “allergy” is called “hay fever”. In GNM terms, the combination of the symptoms indicates that the healing phases of a scent or stink conflict and a visual separation conflict (“I don’t want to see this!”) run concurrently.
|