
DEVELOPMENT AND FUNCTION OF THE PERIOSTEUM: The periosteum covers the outer surface of all bones, except the joints, which are capped with cartilage, and sites that attach to muscles, ligaments, and tendons. It consists for the most part of connective tissue (see also periodontium of the teeth). At first, the periosteum was lined with squamous epithelium. After the muscles, ligaments, tendons and two skin layers ( corium skin and epidermis) had given new support to the bones, the epithelial layer degenerated (in the fetal development this process occurs during the first two weeks of gestation). What remained was a sensitive network of nerves. The neural network of the periosteum has two layers: a lower layer, which registers the pain caused by the swelling of a healing bone, and an upper layer that generates rheumatic pain. The periosteal nerves originate from the ectoderm and are therefore controlled from the cerebral cortex. The innervation of the entire periosteum originates in the spinal marrow of the cervical spine.
|
|
BRAIN LEVEL: The periosteal nerves are controlled from the post-sensory cortex (part of the cerebral cortex). The periosteal nerves of the right side of the body are controlled from the left side of the cortex; the periosteal nerves of the left side of the body are controlled from the right cortical hemisphere. Hence, there is a cross-over correlation from the brain to the organ (see GNM diagram showing the post-sensory homunculus).
NOTE: The periosteal nerves of the dura mater (see meninges) are controlled from the pre-motor sensory cortex.
|
BIOLOGICAL CONFLICT: The biological conflict linked to the periosteum is a severe separation conflict.
In comparison to the separation conflict related to the skin, the conflict linked to the periosteal nerves is experienced as more dramatic, even as brutal or cruel. Depending on the exact conflict situation, the separation might be associated with the arms (not being able to hold a beloved person or a pet), hands (a loved one slipped away), legs and ankles (wanting to push someone away), or feet and toes (an unwanted move). The periosteal nerves lining the eye socket correlate to a visual separation conflict (having lost sight of someone). Like with the epidermis, the conflict also corresponds to wanting to separate from a person or a place.
NOTE: The separation conflict related to the periosteal nerves only refers to a separation from a person or from an animal such as a pet but not to objects (jewelry, car, house) or a separation, let’s say, from a home (see territorial loss conflict).
|
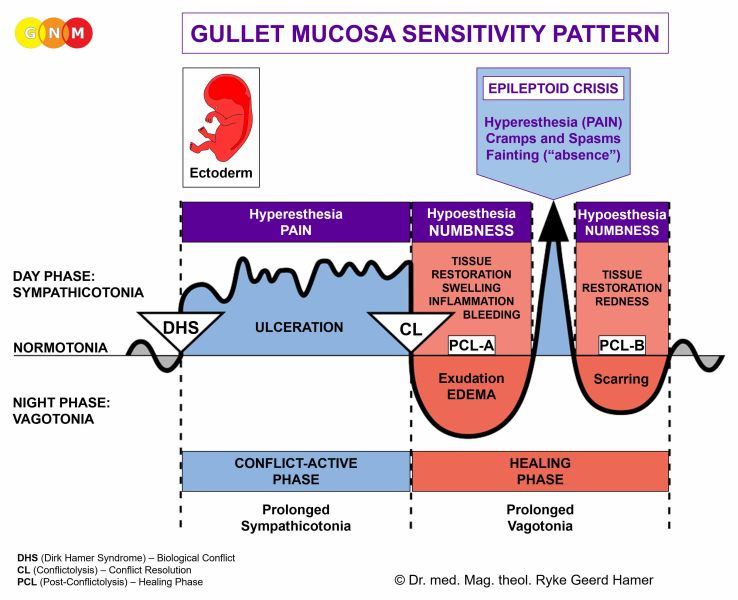
CONFLICT-ACTIVE PHASE: hypersensitivity of the affected part of the body. Conflict activity with a separation conflict is always accompanied by a short-term memory loss, which serves the purpose to forget temporarily the one who has left by blocking out the memory (see also Biological Special Program related to the skin).
The symptoms include a sensation of tingling and sharp, stinging pain (“pins and needles”). The neuralgic pain is commonly referred to as rheumatism (compare with acute joint rheumatism). There might also be a soreness to touch. Severe or long-lasting pain can trigger a self-devaluation conflict involving the underlying bone causing rheumatic pain in the healing phase. In GNM, we call the combination of the two Biological Programs the “ Bone Syndrome”. Pain reaching into the muscle tissue generates soft tissue rheumatism (compare with fibromyalgia). Also, the affected part of the body feels cold (“cold” muscle pain points to conflict activity related to the periosteum whereas “hot” muscle pain is a sign that the muscle itself is healing). This is why warming the area is soothing and alleviates the pain.
NOTE: Whether the right or left side of the body is affected (or both) is determined by a person’s handedness and whether the conflict is mother/child or partner-related. A localized conflict involves the part that is associated with the separation conflict.
|
|
|
This CT scan shows the impact of a severe separation conflict in the post-sensory cortex, precisely, in the areas that control the right and left hand and fingers. The Hamer Focus on the right side is noticeably larger than the one on the left ( view the GNM diagram). The sharp borders reveal conflict activity, hence, the stinging, rheumatic pain in both hands (more in the left hand than in the right). |
The periosteum and the arteries are both innervated from the sympathetic trunks. Hence, during conflict activity ( sympathicotonia) of a separation conflict involving the periosteum, the capillaries become narrow causing a restricted blood circulation.
|
| During conflict activity, the affected area shows reddish-purple bumps similar to frostbites that occur as a reaction to the exposure to frigid temperatures. The medical term for the condition is chilblains or pernio (the Latin word for frostbites). Chilblains on the toes could be caused by the distress of having to separate or wanting to separate from a certain place (the ground one walks on). The condition can involve the top and/or bottom of the toes.
|
|
| With an intense conflict, the affected area(s) turn white due to the reduced blood flow. This condition is termed Raynaud’s disease (compare with peripheral artery disease). |
|
| If the conflict persists over a long period of time, the tissue eventually dies resulting in gangrene.
NOTE: The amputation of the affected limb does not necessarily remove the pain. A rheumatic phantom pain will occur as long as the person is conflict active (see also phantom limb pain involving the bones).
|
The periosteal nerves are part of the peripheral nervous system. In conventional medicine, the nerve pain as well as the numbness are referred to as “peripheral neuropathy”. It is a wide-spread belief that high blood sugar causes damage to the arteries and “indirectly” to the nerves resulting in pain or a loss of sensation, especially in the extremities. Yet, not every diabetic develops the condition! Neither can this assertion explain why an elevated glucose level would, for example, affect the feet (or just one foot or toe) in one person and the arm(s) in another. Based on the knowledge of GNM, what is called “diabetic peripheral neuropathy” is a combination of two Biological Special Programs running simultaneously: one involves the beta islet cells of the pancreas linked to a “ resistance conflict” causing diabetes, the other involves the periosteum related, in case of the legs, to “wanting to kick somebody away” (usually the person one resists) with the development of leg ulcers or gangrene, depending on the intensity and duration of the conflict (see also “diabetic retinopathy”).
Trigeminal neuralgia occurs when the separation conflict was associated with the face, either literally (loss of “cheek”-contact) or figuratively (a “slap in the face”). The sharp, electric-like pain along the trigeminal nerve innervating the face is brief but strong and might reoccur many times over the course of the day. The condition is usually confined to one side (see also trigeminal neuralgia related to the facial bones and to the facial skin).
NOTE: The trigeminus nerve has sensory and motor branches. The motor branch of the nerve is affected by facial paralysis.
|
HEALING PHASE: hyposensitivity. Because of the loss of sensitivity the affected part of the body (hands, arms, legs, feet) feels numb (compare with hyposensitivity related to the epidermis and a loss of sensation, for example in the lower extremities, due to a compression of a spinal nerve).
The short-term memory loss reaches into PCL-A. For the period of the Epileptoid Crisis, the rheumatic pain returns; typically during the night hours. During PCL-B, the sensitivity slowly normalizes, provided there are no conflict relapses causing pain flare-ups.
PERIOSTEUM - TRANSLATIONS
|
| <---- In these PDF documents you can enlarge images. If your browser cannot handle this desirable feature, then you will need to download and install the authentic Adobe Acrobat Reader. |
Click on the icon to download the PDF file
|
English Original
|
Catalan Translation
|
Dutch Translation
|
|
French Translation
|
Serbian Translation
|
Spanish Translation
|
|
|












{kind=link}