Female Sexual Organs
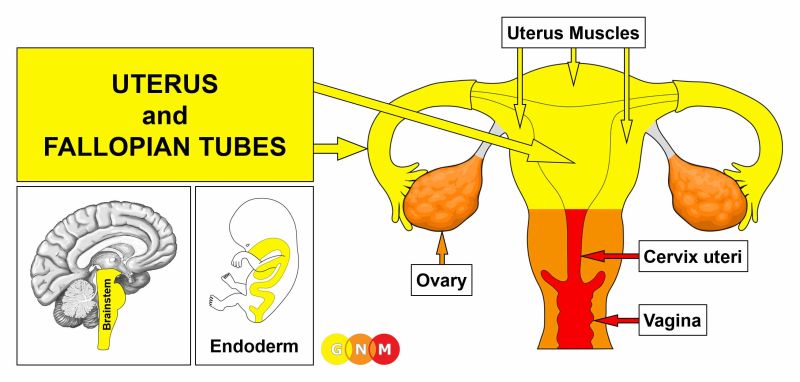
DEVELOPMENT AND FUNCTION OF THE UTERUS AND FALLOPIAN TUBES: The uterus (corpus uteri) is located in the female pelvis behind the urinary bladder. The uterus is held in place by ligaments. The outer layer of the uterus (perimetrium) consists of a peritoneal membrane that gives additional support to the organ. Throughout the menstrual cycle, the endometrium (inner lining of the uterus) grows a tissue layer rich of blood vessels to provide an optimum environment for an embryo. If the fertilization of the egg does not occur the endometrial lining is shed and expulsed during menstruation. The uterus opens into the vagina through the cervix, or “neck of the uterus” (cervix uteri). Two fallopian tubes connect the uterus with the ovaries. The tubes produce a secretion (secretory quality) that aids to carry sperm and the fertilized ovum to the uterus, where the blastocyst adheres to the endometrium. Next to nourishing the developing fetus, the uterus secretes prostaglandin (secretory quality), a hormone-like substance that stimulates uterine contraction at the beginning of labor. The uterus and fallopian tubes consist of intestinal cylinder epithelium, originate from the endoderm and are controlled from the brainstem.
NOTE: At first, the female reproductive system had two uteri that eventually grew together forming one single organ. Two uteri also form initially in the human embryo fusing into a single uterus during the development of the female fetus. The same process takes place with the originally two bladders.
|
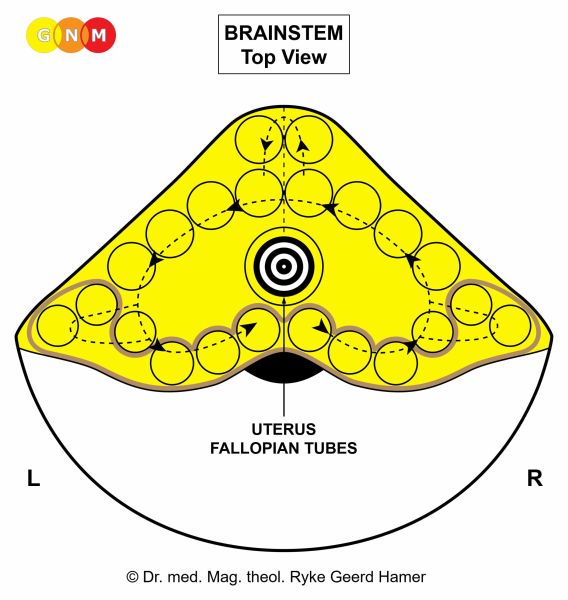
BRAIN LEVEL: The uterus and fallopian tubes are controlled from the center of the brainstem.
NOTE: The uterus, fallopian tubes, and the prostate gland share the same brain relay.
BIOLOGICAL CONFLICT: The biological conflict linked to the uterus and fallopian tubes is a procreation conflict (equal to the prostate-related conflict in males) or an “implantation conflict” (compare with mating conflict related to the cervix uteri). Hence, a miscarriage, an abortion, not getting pregnant (see also uterus muscles) as well as the loss of a child or grandchild (compare with loss conflict related to the ovaries) can trigger the conflict. In addition, the uterus and fallopian tubes correspond to a gender conflict experienced as an “ugly conflict with a male”. Feeling humiliated by a man (physical, sexual, or emotional abuse), verbal insults, disrespectful treatment by a partner, spouse, male relative or friend, offensive behavior of a colleague, or harassment by a former boyfriend, ex-spouse (after an “ugly” divorce), or a male authority (supervisor, doctor, judge, policeman, etc.) are possible conflict scenarios. A distressing gynecological exam could also provoke the conflict.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the uterus proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to thicken the uterus mucosa to aid the implantation of the fertilized egg.
Painful menstrual periods: The contraction of the uterus muscles is stimulated by the hormone prostaglandin that is produced in the uterus mucosa. The overproduction of prostaglandin during the conflict-active phase of a procreation or gender conflict causes the uterus to contract more strongly than normal, resulting in painful menstrual cramps (see also painful menstruation linked to the Biological Special Program of the ovaries).
|
With prolonged conflict activity (hanging conflict) a cauliflower-shaped growth (secretory type), referred to as a uterus cancer (endometrial cancer), forms as a result of the continuing cell augmentation. If the rate of cell division exceeds a certain limit, conventional medicine considers the cancer as “malignant”; below that limit, the growth is regarded as “benign” or diagnosed as a uterine polyp (see also healing phase). A growth that develops on a flat plane is termed endometrial hyperplasia (the same diagnostic standard is applied to prostate cancer and prostate hyperplasia). There are no symptoms during the conflict-active phase. In the fallopian tubes, however, a compact growth (secretory type) might temporarily obstruct the affected tube causing pain, especially during ovulation (also in the healing phase).

On this brain CT, we see a Hamer Focus in the uterus relay (view the GNM diagram) corresponding to a uterus cancer. The Hamer Focus in the control center of the liver (on the right brainstem hemisphere) shows the impact of a starvation conflict, which occurred most likely together with the conflict related to the uterus.
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. The healing process is accompanied by night sweats. When fungi assist healing, this causes uterine candidiasis (compare with vaginal candidiasis related to the Bartholin’s glands). The discharge produced during the cell (tumor) breakdown is excreted through the vagina. The discharge is white (cheese-like), has a distinct foul-smelling odor, and might contain blood. NOTE: The “vaginal discharge” originates in the uterus or fallopian tubes and not, as assumed, in the vagina since the vaginal canal is not endowed with an endodermal submucosa and subsequently not populated by fungi or bacteria.
Endometritis (not to be confused with endometriosis) is an inflammation in the uterus with painful swelling. With concurrent water retention (the SYNDROME) as a result of an active abandonment or existence conflict, the swelling increases and so does the pain. In the fallopian tubes, the swelling could temporarily block the affected tube (see also conflict-active phase). Since the fallopian tubes are permeable, the discharge produced during the decomposing process might leak into the abdominal cavity. A tubal inflammation is called salpingitis or adnexitis (the same medical term is used for an inflammation of the ovaries). Whether the conflict affects the right or left fallopian tube is random.
With an intense healing phase the outer wall of the uterus tumor might break resulting in acute bleeding or hemorrhaging, particularly during menstruation when the tumor removal concurs with the shedding of the decidua (endometrial lining). Hence, heavy menstrual bleeding (menorrhagia) might point to relapses (tracks) of a uterus-related conflict (see also heavy periods related to uterus muscles, ovaries, cervix uteri, and manic depression). Light bleeding accompanies healing when the preceding conflict activity was less intense or if a woman is already postmenopausal or is not menstruating at the time when healing takes place.
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells remain. Eventually, the growth becomes encapsulated with connective tissue. In conventional medicine, this is usually diagnosed as a “benign cancer” or a uterine polyp (see also conflict-active phase).
UTERUS and FALLOPIAN TUBES
|

DEVELOPMENT AND FUNCTION OF THE UTERUS MUSCLES: The middle layer of the uterus, known as the myometrium, makes up most of the uterus volume. The myometrium is for the most part composed of smooth muscles. The main function of the uterus muscles is to hold the fetus and to aid its delivery during childbirth. The hormone oxytocin, produced in the pituitary gland, induces the contraction of uterus muscles during labor. The uterus muscles derive from the endoderm and are controlled from the midbrain.

BRAIN LEVEL: The uterus muscles are controlled from the midbrain, located at the outermost part of the brainstem.
BIOLOGICAL CONFLICT: The biological conflict linked to the uterus muscles is “not being able to hold the fetus” (complications during pregnancies, miscarriages, abortions; see also cervical muscles) or not getting pregnant (compare with procreation conflict related to the uterus). Hence, not being able to have children because of an early menopause, the removal of both ovaries, infertility, a mate’s infertility or erectile dysfunction, difficulties conceiving, or an unfulfilled desire to have (more) children are typical conflict situations. Having the “tubes tied” (tubal ligation), the use of an IUD to prevent pregnancy, or taking contraceptives might evoke the conflict on a subtle psycho-biological level. A woman can experience the conflict also with or on behalf of a female member of the group (her daughter or granddaughter, a close female relative or friend).
CONFLICT-ACTIVE PHASE: cell proliferation with the formation of uterine fibroids (fibromyomas or leiomyomas). The biological purpose of the additional muscle tissue is to increase the tension (hypertonus) and to strengthen the uterus muscles in order to be better able to hold the fetus or to facilitate delivery. The size of the fibroid(s) is determined by the degree and duration of conflict activity.
HEALING PHASE: The muscle tension normalizes. However, to secure procreation the fibroids remain past the completion of the healing phase.

Fibroids located close to the endometrium of the uterus can cause acute bleeding, particularly during the Epileptoid Crisis, and heavy menstrual periods since the fibroids are covered by the endometrial lining that is shed during menstruation (see also heavy periods related to uterus mucosa, ovaries, cervix uteri, and manic depression).
With the SYNDROME, that is, with water retention as a result of an active abandonment or existence conflict involving the kidney collecting tubules, the retained water increases the size of the fibroid(s). A large growth in the uterus musculature might be diagnosed as a myometrial sarcoma.
Uterine prolapse: The uterus is also held in place by ligaments. A lasting self-devaluation conflict (“I am not good enough there!”) weakens the structures causing the uterus to descend into the vaginal canal.
PREGNANCY AND CHILDBIRTH
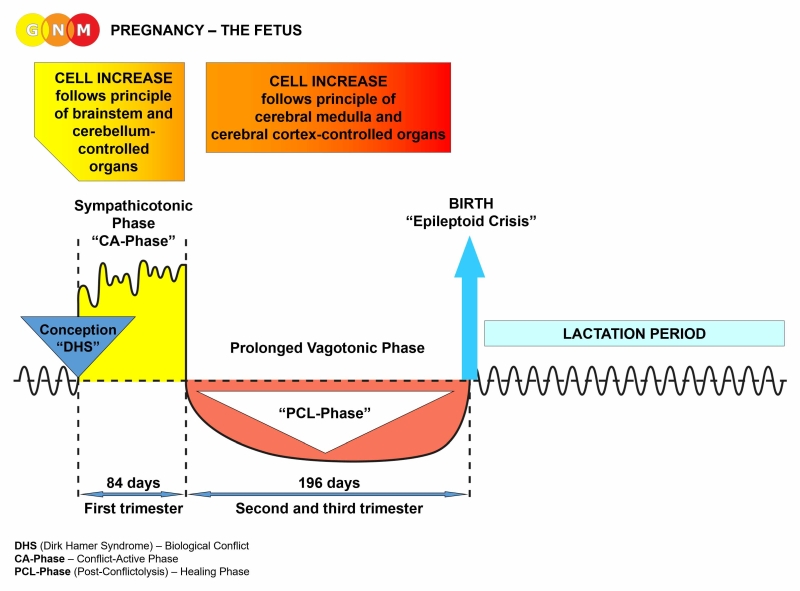
 Similar to a Biological Special Program that is initiated by a biological conflict, the pregnancy – the period from conception to birth – progresses in two phases: a sympathicotonic phase followed by a vagotonic phase. The moment of conception is equivalent to a DHS.
In human females, the pregnancy lasts around 280 days (little more than 9 months) or 40 weeks, calculated from the beginning of the last menstrual period. The first trimester (sympathicotonic phase) lasts 84 days (12 weeks); the second and third trimester (vagotonic phase) lasts 196 days (28 weeks). The two phases proceed synchronously in the organism of the mother and the fetus.
THE DEVELOPMENT OF THE FETUS
 Starting with the first cell division after conception, the embryo grows into a cluster of cells, called a blastocyst. The outer cell layer of the blastocyst (trophoblast) connects with the endometrium of the uterus to facilitate the implantation of the egg and the formation of the placenta. The inner cell mass of the blastocyst (embryoblast) is responsible for the formation of the embryo itself. Within two weeks, the blastocyst divides into three embryonic germ layers (endoderm, mesoderm, ectoderm). Over the course of gestation, the embryonic germ layers develop all organs and tissues of the human body through continuous cell division.
During the first three months, the fetus is in a state of sympathicotonia (“CA-Phase”). The development of the fetus follows the principle of brainstem and cerebellum-controlled organs with cell increase in the sympathicotonic phase. This is in accordance with a Biological Special Program that generates cell proliferation during the conflict-active phase. It is the period (“CA-Phase”) when, for example, the organs of the intestinal canal and the lungs develop. NOTE: The biological handedness of the fetus is established at the moment of the first cell division after conception.
The vagotonic phase starts at the fourth month of pregnancy and lasts until birth. During the vagotonic phase, the development of the fetus follows the principle of cerebral medulla and cerebral cortex-controlled organs with cell increase in vagotonia. This is in accordance with a Biological Special Program that generates cell proliferation during the healing phase, precisely during PCL-A.
The birth process is equal to the Epileptoid Crisis.
After birth, the newborn enters the lactation period.
THE PREGNANT WOMAN
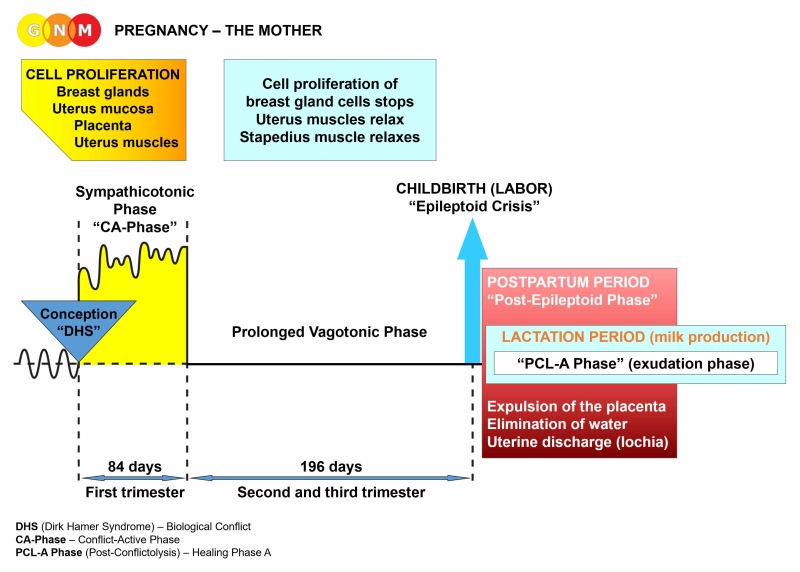 Like the fetus, during the first three months of pregnancy, the mother is in a state of sympathicotonia (“CA-Phase”). According to the principle of brainstem and cerebellum-controlled organs, during the sympathicotonic phase, cell proliferation occurs
Throughout the sympathicotonic phase, the pregnant woman tends to be restless and nervous. Nausea is a sympathicotonic symptom. This is why morning sickness occurs during that period.
At the beginning of the vagotonic phase that lasts from the fourth month of pregnancy to childbirth, the proliferation of breast gland cells stops. The breasts continue to get bigger; not because of cell increase of breast gland cells but rather due to the increased storage of fat in the breasts. Throughout the vagotonic phase the uterus muscles relax in order to prevent a premature birth. The stapedius muscle, located in the middle ear, is a muscle that is fundamental in sound transmission. In vagotonia, when we sleep, the stapedius muscle is relaxed so that we become instantly aware of the slightest noise. During pregnancy, this noise sensitivity protects the mother and her baby from potential danger. Being in vagotonia, the pregnant woman has good appetite in order to be able to provide herself and the growing fetus with sufficient amounts of food. In the vagotonic phase, the pregnant woman tends to be tired, which serves the purpose to prevent the mother from exerting herself and not to put herself and her baby in danger. The vagotonic state of the mother provides the unborn child with the optimum condition for its development.
LABOR AND CHILDBIRTH
The birth of the child that takes place at the end of the vagotonic phase (“PCL-A”) is equivalent to the Epileptoid Crisis. With the beginning of labor, the mother and the fetus are pulled out of vagotonia and enter a heightened sympathicotonic state, as it happens during the Epileptoid Crisis of a Biological Special Program. Mother and child go through the process together.
The “Epileptoid Crisis” of the mother presents as labor contractions. Starting at the onset of labor, the uterus muscles contract (prolonged tonic cramps) with simultaneous rhythmic, clonic, peristaltic motions to facilitate delivery. From an evolutionary point of view, the tonic-clonic labor contractions became the blueprint for the Epileptoid Crisis that occurs at the height of the Biological Special Program of the striated muscles. Together with the contraction of the uterus muscles, the internal uterine orifice and the cervical sphincter open (sphincters open in sympathicotonia). The baby is pushed through the vaginal canal through the concerted peristaltic motion of the uterus muscles, cervical muscles, and vaginal muscles. The average length of labor is about eight hours.
The “Epileptoid Crisis” of the fetus presents as tonic muscle contractions that make the body stiff, which allows the fetus to move easier through the birth canal.
Labor and childbirth constitute the end of pregnancy.
THE POSTPARTUM PERIOD
Right after labor and childbirth the organism of the mother enters the postpartum period or a “Post-Epileptoid Phase” with the expulsion of the placenta and the elimination of large amounts of water through the kidneys – similar to the “urinary phase” that occurs immediately after the Epileptoid Crisis of a Biological Special Program.
During the postpartum period, the additional cells of the uterus mucosa that had thickened the uterus during pregnancy are removed with the help of TB bacteria. TB bacteria clean the uterus! The tubercular discharge from the uterus (called lochia) contains blood, mucus, and remnants of the placenta. The post-birth uterine discharge lasts about 4-6 weeks.
A postpartum infection of the uterus (endometritis) accompanied by fever is known as “childbed fever” (puerperal fever). Conventional medicine claims that the infection is caused by bacteria that enter the uterus through the vagina. Some even suggest that the infection spreads to the uterus “from a sore throat or infected gums or from the anus during delivery” (Source). Another theory proposes that the infection is transmitted to the pregnant woman from doctors or nurses through contact with other patients. Based on the Fourth Biological Law and the beneficial role of microbes, “infections” are not transmittable from person to person; microbes only work in organs and tissues that are healing at the time. Hence, from a GNM point of view, the enhanced microbial activity in the uterus following childbirth indicates a healing phase of a uterus-related conflict such as a gender conflict (an ugly conflict with a male).
Mental conditions after childbirth: see postpartum depression and postpartum psychosis
LACTATION PERIOD
With the birth of the child, the mother enters the lactation period. The breast gland cells that multiplied in the first trimester change from a non-secretory to a secretory state. The milk production during the “PCL-A” or exudation phase is equivalent to the fluid production as it occurs in the PCL-A phase of a Biological Special Program. Hence, after childbirth, the organism of the mother continues the biological program where it had left after the first trimester (“CA-Phase”).
An increase, reduction, or cessation of milk production relates to the prolactin producing cells in the pituitary gland (controlled from the brainstem). Prolactin stimulates the breast glands to produce milk. The corresponding biological conflict is a feeding conflict as in “not being able to nourish the child” (for example, due to financial difficulties of an unemployed or self-employed single mother or unemployed spouse or partner). In the conflict-active phase, the prolactin producing cells proliferate in order to produce more milk for the baby. The overproduction of prolactin causes an increased milk production. After the conflict has been resolved, the additional cells are removed with the help of fungi or TB bacteria. With a hanging healing more and more glandular tissue gets lost as a result of the continuous cell removal process. In nursing females, this causes a reduction or cessation of milk production. If the prolonged healing phase started already during the time of pregnancy, a woman has little or no breast milk after the delivery of her child. The distress of not producing enough milk can trigger a fluid conflict involving the kidney parenchyma with hypertension (see pre-eclampsia).
A reduction or cessation of milk production relates also to the Biological Special Program of the breast glands (controlled from the cerebellum) linked to a nest-worry conflict associated with a nest-member, including the newborn. In the conflict-active phase, the breast gland cells proliferate in order to produce more milk. Hence, during conflict activity, the nursing mother has more milk in the affected breast (see handedness). In the healing phase, the additional cells are removed with the help of fungi or TB bacteria. When the healing phase is prolonged, the ongoing decomposing process leads to a loss of breast gland cells. If a woman is nursing at the time, the loss of glandular breast tissue causes a reduced or complete stop of milk production in the affected breast.
In breastfeeding women, lactation mastitis or an inflammation of the nipple (thelitis) is linked to a separation conflict (for example, due to a separation from the baby after birth) or “wanting to separate” from the nursling because the baby is sucking too strong. In the healing phase, the area of the affected milk ducts becomes inflamed.
Biological conflicts experienced by the MOTHER
When a pregnant woman suffers a biological conflict during the first trimester (sympathicotonic phase), the corresponding organ generates cell proliferation or cell loss, depending on the nature of the conflict. At the beginning of the fourth month of pregnancy (vagotonic phase), the changes on the organ level stop. The conflict is not resolved, only postponed! If the conflict has not been resolved by the time of delivery, the cell increase or cellular depletion on the affected organ continues with the onset of labor (“Epileptoid Crisis”). A reactivation of a conflict or of several conflicts can create a postpartum depression or postpartum psychosis.
The sympathicotonic state of the mother in the first trimester explains why healing symptoms that she had before she got pregnant, for example a skin condition, are alleviated or stop completely during the first three months of pregnancy because sympathicotonia interrupts healing. If she has a conflict relapse of a separation conflict in the first trimester, she will not get a rash outbreak.
A strong DHS (intense sympathicotonia) can cause a miscarriage (increased sympathicotonia opens the cervical sphincter). Most miscarriages occur during the first three months of pregnancy.
If the mother was conflict-active before she got pregnant, the changes on the related organ also stop once she enters the fourth month of pregnancy. In case she has not resolved the conflict by the time of delivery, the conflict will be fully reactivated with the beginning of labor.
When a pregnant woman suffers a biological conflict during the second or third trimester (vagotonic phase), the conflict doesn’t play out as it normally would. Throughout the vagotonic phase, the conflict intensity is significantly downgraded; hence, the cell proliferation or cell loss of the conflict-related organ is also reduced. The same applies to schizophrenic constellations as well as to conflict relapses. If the mother has a relapse of a conflict she carried into her pregnancy or of a conflict she experienced in the first trimester, the intensity of the symptoms is reduced throughout the vagotonic phase. However, with the onset of labor (“Epileptoid Crisis”), which constitutes the end of pregnancy, the mother is in full conflict activity. NOTE: A woman with a maturity stop is able to catch up in her emotional development during the last six months of pregnancy.
A strong DHS (sympathicotonic state) interrupts the vagotonic phase causing a premature birth (the cervical sphincter opens in sympathicotonia). The same happens with a strong Epileptoid Crisis, particularly when the heart or lungs are involved. NOTE: When the mother is highly conflict active (in great panic) or suddenly in an intense constellation, the vessels supplying the placenta are narrowed, depriving the baby of oxygen and nutrients. This can result in acute complications and death of the fetus (stillbirth).
If the mother resolves a conflict that occurred before pregnancy or in the first trimester, during the vagotonic phase she develops the corresponding symptoms, for example, a cold (stink conflict), diarrhea (indigestible morsel conflict), a skin rash or herpes (separation conflict), varicose veins (ball-and-chain conflict), hepatitis (territorial anger conflict), or any type of cancer such as a lymphoma, colon cancer, or leukemia that arises in the healing phase. Concurrent water retention due to an abandonment or existence conflict (the SYNDROME) involving the kidney collecting tubules exacerbates the healing symptoms! After resolving an overwhelmed conflict or territorial loss conflict, she will suffer a heart attack during the Epileptoid Crisis. A strong Epileptoid Crisis could put the life of the mother and the unborn in danger. Concerning infections such as a bladder infection (territorial marking conflict) or a “vaginal” yeast infection (gender conflict), the infection of the mother cannot be transmitted to the newborn, as claimed by conventional medicine, because the “infection” is already a healing symptom (see Fourth Biological Law).
Symptoms during pregnancy
Pre-eclampsia: In conventional medicine, the term pre-eclampsia is used when the pregnant woman has high amounts of protein in the urine or when her blood pressure is elevated. It is considered a “multi-system disorder specific to pregnancy”. Based on GNM, high amounts of protein in the urine occur in the vagotonic phase of pregnancy, after an abandonment or existence conflict has been resolved (see proteinuria and albuminuria related to the kidney collecting tubules). Elevated blood pressure is linked to a fluid conflict, for example related to the amniotic fluid (“something is wrong with the amniotic fluid”) or an overwhelmed conflict involving the right myocardium (see hypertension in conflict-active phase and PCL-A).
Maternal Anemia: During the vagotonic phase, general fatigue is normal. The fatigue of anemia, however, is caused by a self-devaluation conflict brought on by humiliation, abuse, or an association with the pregnancy itself (see anemia in the conflict-active phase and healing phase).
Vomiting in the second and third trimester: Vomiting occurs during the Epileptoid Crisis of a territorial anger conflict involving the small curvature of the stomach or of an indigestible morsel conflict related to the upper part of the small intestine. Hence, in the vagotonic phase of pregnancy! Recurring vomiting episodes are provoked by setting on a conflict-related track (compare with morning sickness in the first trimester).
Gestational diabetes: Gestational diabetes develops as a result of a male resistance conflict that occurred during pregnancy. NOTE: When a woman is pregnant or breast feeding her estrogen status is low, she therefore experiences conflicts like a male.
Biological conflicts experienced by the FETUS
The fetus can suffer biological conflicts just as much as a newborn, infant, child, or an adult. In accordance with the formation of the three embryonic germ layers, the fetus can only experience conflicts that correlate to organs that have already developed, i.e., initially only conflicts that correlate to organs deriving from the endoderm and old mesoderm such as a death-fright conflict, starvation conflict, or attack conflict.
When the fetus experiences a biological conflict during the first three months (sympathicotonic phase), the corresponding organ generates cell proliferation in the conflict-active phase. At the beginning of the fourth month of the fetal development (vagotonic phase), the cell augmentation stops. However, with the beginning of the birth process (“Epileptoid Crisis”), the newborn becomes fully conflict active and the cell increase on the affected organ continues.
A strong DHS with intense conflict activity (sympathicotonic state) can cause a miscarriage (the fetus aborts itself) and the pregnancy comes to an end. The adrenals of the fetus that develop in the fifth week secrete cortisone that stimulates the production of oxytocin (see pituitary gland), which induces the contraction of the uterus muscles.
When the fetus experiences a biological conflict during the second or third trimester (vagotonic phase), for example a separation conflict or territorial anger conflict, the conflict intensity is significantly reduced. In case of ongoing conflict activity (hanging conflict), with the beginning of the birth process (“Epileptoid Crisis”), the baby becomes fully conflict active.
If the fetus resolves a conflict during the vagotonic phase, the baby is born with the organ-related healing symptoms. The symptoms last until the Biological Special Program is completed. NOTE: Congenital anomalies or birth defects presenting at birth such as physical or structural anomalies or malformations of an organ (spina bifida, cleft lip or cleft palate, absence of a nasal bone, abnormal limbs, heart defects) are unrelated to a biological conflict.
Intrauterine conflicts
Lacking visual perception, the fetus perceives predominantly sounds and noises. Pregnant women often feel a jerk or kick from the baby following a sudden loud noise, like a door slam. Loud noises, for example, from noisy machines such as saws (chain saw, table saw), drilling tools, jackhammers, or lawn mower, loud street noise from trucks or motor cycles, ear-piercing music, loud bangs or blasts, blaring sirens, noisy kitchen equipment (blender) held close to the belly, but also yelling and screaming in the immediate environment (the mother yelling at her other children, loud arguments between the parents), or the loud barking of a dog can put the fetus into panic causing a DHS in the unborn. Also, a fetus can suffer a biological conflict through the exposure to ultrasound. Research has shown that the noise of ultrasound puts the fetus into an agitated state (Source: “The quality of fetal arm movements as indicators of fetal stress”, PubMed, 2010). In the womb, any noises are perceived particularly loudly because the fluid in the amniotic sac is a much stronger sound conductor than air.
Loud noises can cause a …
Self-devaluation conflict: The unborn can suffer a self-devaluation conflict when it feels unwanted. After the resolution of the conflict during pregnancy or after birth, the child develops leukemia. A slow mineralization of the bones (“weak bones”) as a result of a hanging healing is termed rickets. Rickets affects the skull (“This is not fair!”), arm, legs, spine, or the entire skeletal system (generalized self-devaluation conflict). The theory that rickets is caused by a vitamin D deficiency is pure assumption.
Fear of suffocating: The baby can suffer a fear of suffocation when the umbilical cord is wrapped around the neck (nuchal cord) caused by agitated fetal movements (see exposure to ultrasound). The conflict involves the goblet cells of the bronchia (controlled from the same brain relay as the lung alveoli in the brainstem). During the conflict-active phase, the goblet cells increase in number in response to the distress of not getting enough air. In the healing phase, the additional cells are broken down with the help of TB bacteria. If the healing process is continuously interrupted by conflict relapses, this causes mucoviscidosis in the bronchi or so-called cystic fibrosis. The same can occur when the umbilical cord is cut too early because the lungs of the newborn need a certain amount of time to get used to independent breathing.
Sudden Infant Death Syndrome (SIDS): The sudden death of the baby usually happens during sleep (in vagotonia) between the first and sixth months of life. According to GNM, death occurs when the baby goes into the healing phase of several conflicts experienced during gestation or after birth. Death is caused by the pressure of the brain edemas, particularly with the SYNDROME, an active abandonment or existence conflict.
|

DEVELOPMENT AND FUNCTION OF THE FEMALE GERM CELLS: In the human reproductive organs, germ cells are the cellular units that give rise to gametes (eggs and sperms). The primordial germ cells appear first in the yolk sac of the embryo from where they migrate through the developing intestine to the new gonads (testicles or ovaries). In the ovaries, the germ cells form so called oogonia (secretory quality) that are precursor cells of oocytes from which an egg or ovum develops. This process, called oogenesis, takes place during the development of the fetus. Thus at birth, the female infant is born with the entire number of eggs (in males, spermatogenesis, the production of sperms, continues throughout life). Starting with puberty, each month during ovulation a mature egg is released into the fallopian tube for fertilization (ovulation is stimulated by the LH-Luteinizing Hormone produced in the pituitary gland). After the discharge of the ovum, the corpus luteum (“yellow body”), a hormone-producing cell cluster in the ovaries, secretes progesterone that helps to prepare the uterus and uterus muscles for pregnancy and to maintain gestation. It also plays a role in the development of the breast glands in preparation for nursing (this is why progesterone in birth control pills leads to breast growth). The corpus luteum as well as the germ cells derive from the endoderm and are controlled from the midbrain.
BRAIN LEVEL: The female (and male) germ cells are controlled from the midbrain, located at the outermost part of the brainstem. The germ cells in the right ovary are controlled from the right side of the midbrain; the germ cells in the left ovary from the left side (compare with interstitial cells of the ovaries).
BIOLOGICAL CONFLICT: The biological conflict linked to the germ cells is a profound loss conflict, often the loss of a child (compare with loss conflict related to the ovaries).
CONFLICT-ACTIVE PHASE: During the conflict-active phase an ovarian teratoma (secretory type), or germ cell tumor, develops from the corpus luteum (see also testicular teratoma in males). The significance of a teratoma relates to the primeval ability of parthenogenesis, the reproduction without fertilization. The biological purpose of the additional germ cells is to facilitate faster reproduction in the emergency of the loss of an offspring. In conventional medicine, a “malignant teratoma” is classified as an ovarian cancer (compare with “ovarian cancer” related to the ovaries).
NOTE: The cell proliferation that takes place with the growth of a teratoma is the same as it occurs in the development of the fetus. During the first three months of pregnancy, the cell increase follows the principle of old brain-controlled organs with cell proliferation in sympathicotonia (conflict-active phase). Starting at the fourth month of gestation, the cell proliferation follows the pattern of cerebrum-controlled organs with cell proliferation in vagotonia (healing phase).
|
HEALING PHASE: With the conflict resolution (CL) the teratoma stops growing only slowly since embryonic tissue develops in spurts (“fetal growth spurt”). During the healing phase, fungi or mycobacteria such as TB bacteria may decompose the teratoma, provided they are available. The swelling filled with pus presents as an ovarian abscess. The healing process is accompanied by night sweats. If the teratoma remains, the growth encapsulates. Remarkably, an encapsulated teratoma, termed a dermoid cyst, might contain structures such as hair, teeth, or bones.

DEVELOPMENT AND FUNCTION OF THE OVARIES: The ovaries are located at the right and left side of the uterus to which they attach through cord-like ligaments. During a woman’s monthly cycle, an egg, formed from primordial germ cells, grows into a tiny sac, called a follicle. At the time of ovulation, the follicle breaks open allowing the ovum to be released and travel from an ovary through the fallopian tube to meet a sperm for fertilization. After about six days, the fertilized egg or blastocyst implants in the uterine cavity. The corpus luteum, a progesterone-producing cell cluster in the ovaries, facilitates pregnancy. The ovarian tissue contains interstitial cells resembling those of the testicles. The interstitial cells are responsible for the production of estrogen and small quantities of testosterone. Estrogen plays a significant role in a woman’s sex drive and “readiness to mate”. The ovaries originate from the new mesoderm and are therefore controlled from the cerebral medulla.
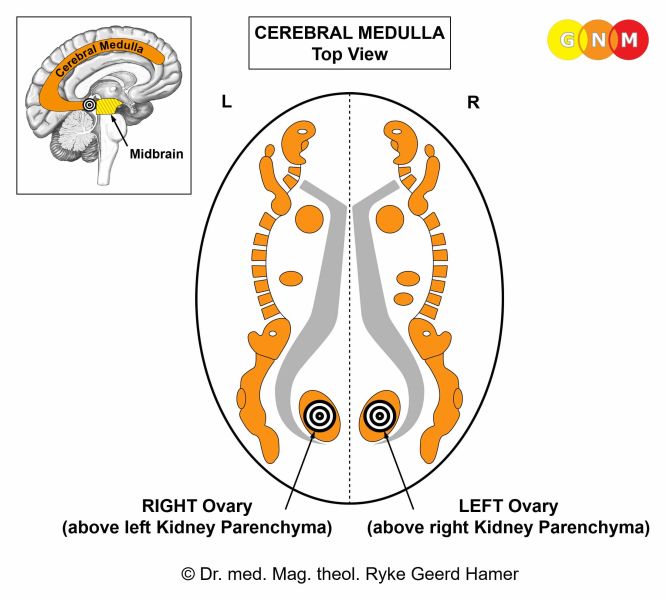
BRAIN LEVEL: The ovaries are controlled from the cerebral medulla, at the area where it adjoins the midbrain. The right ovary is controlled from the left side of the brain; the left ovary is controlled from the right cerebral hemisphere. Hence, there is a cross-over correlation from the brain to the organ.
NOTE: The ovaries and the testicles share the same brain relays.
BIOLOGICAL CONFLICT: The biological conflict linked to the ovaries is a loss conflict concerning the loss of a loved one (see also loss conflict related to the testicles). In comparison, the loss conflict related to the female germ cells is more of a primeval nature. The fear of losing a beloved person can already trigger the conflict. The same holds true for the loss of a pet. Constant self-blame following a break-up or the death of someone close can keep the conflict active. Women also suffer loss conflicts after miscarriages or coerced abortions (compare with implantation conflict related to the uterus). A loss conflict can be activated through an argument, betrayal, or unfaithfulness of a partner or friend. NOTE: The loss conflict related to the ovaries only concerns a person or a pet and NOT the loss of a home (see separation conflict related to the milk ducts).
CONFLICT-ACTIVE PHASE: necrosis (cell loss) in the ovary. Because of the reduction of estrogen-producing cells the estrogen level decreases. Depending on the intensity of the conflict, prolonged conflict activity results in irregular periods, a delayed menarche (first menstruation), amenorrhea (absence of menstruation), or infertility until the conflict is resolved (see also cervix uteri). The “loss” of the unconceived child can lead to lasting infertility.
NOTE: Whether the right or left ovary is affected is determined by a woman’s handedness and whether the conflict is mother/child or partner-related.
|

On this brain scan, we see an active Hamer Focus (sharp target ring) in the area of the brain that controls the right ovary (view the GNM diagram) – compare with brain CT below. For a right-handed female, the related loss conflict is associated with a partner, for a left-handed female with her mother or child.
HEALING PHASE: Following the conflict resolution (CL), the tissue loss is replenished with new cells, ideally assisted by bacteria such as streptococcus bacteria. Healing symptoms are pain caused by the swelling. An inflammation or “infection” of the ovaries is called adnexitis (the same medical term is used for an inflammation of the fallopian tubes).
A special characteristic regarding the healing of the ovaries is the development of an OVARIAN CYST. Provided there are no conflict relapses that interrupt healing, the process takes – like a pregnancy – nine months to complete (see also testicular cyst, kidney cyst, and adrenal cyst). The cyst formation occurs in several steps.
During PCL-A a fluid-filled capsule or cyst forms at the site of the necrosis. With water retention (the SYNDROME) brought on by an active abandonment or existence conflict, an ovarian cyst can become quite large since the retained water is exceedingly stored in the healing area. Large cyst(s) cause considerable pain, particularly during menstruation, and heavy menstrual bleeding (see also uterus mucosa, uterus muscles, cervix uteri, and manic depression). What is termed “polycystic ovaries” (PCO) points to multiple loss conflicts resulting in “many” cysts.
In order to restore the cell loss that occurred during the conflict-active phase, ovarian cells start to proliferate inside the cyst. At this early stage, the cyst attaches itself to neighboring tissue for blood supply; adhering to adjacent tissues also stabilizes the cyst. Detected during this period, the “growth” is diagnosed, in conventional medicine terms, as an “invasive or infiltrating” ovarian cancer (compare with ovarian cancer related to the germ cells) and wrongly assumed to “metastasize” to nearby organs. Based on the Five Biological Laws, the new ovarian cells cannot be regarded as “cancer cells” since the cell increase is, in reality, a replenishing process.
NOTE: Conventional medicine uses a “cancer antigen” called CA 125 as a tumor marker for ovarian cancer. Like the PSA test, the CA 125 screening test is unreliable and inconclusive. “The problem is that while CA 125 is produced by epithelial ovarian cancer cells, it is also made by normal cells. Some people have naturally high levels of CA 125. In many cases, inflammation or irritation of tissues in the abdomen, or conditions including uterine fibroids can cause CA 125 levels to rise. Endometriosis, liver ailments including hepatitis and cirrhosis, and pelvic inflammatory disease can also affect CA 125 levels. On the other hand, 10 to 20 percent of ovarian cancer patients have normal levels of CA 125 when their tumors are diagnosed. One study found that among patients with stage 1 ovarian cancer, fewer than half had abnormal levels of CA 125” (“Special Report: Tumor Marker CA 125”, HoltzReport, December 1997).
|
After the Epileptoid Crisis, the cyst has lost most of its fluid. In PCL-B the cyst becomes hard, separates from the neighboring tissue and, endowed with blood vessels, integrates itself completely into the hormone-producing function of the ovaries. And this is precisely the biological purpose. The boost of estrogen provided by the cyst makes the female who has lost an offspring or a mate more attractive, increasing at the same time her readiness to mate, which puts her into an ideal position to make up for the loss and become pregnant again.
NOTE: All organs that derive from the new mesoderm (“surplus group”), including the ovaries, show the biological purpose at the end of the healing phase. After the healing process has been completed, the organ or tissue is stronger than before, which allows being better prepared for a conflict of the same kind.
|

This brain CT shows swelling (edema) in the brain relay of the right ovary (view the GNM diagram, pushing into the left lateral ventricle. The CT confirms the presence of an ovarian cyst on the organ level (compare with CT scan above).
If the pressure in a liquid or semi-liquid cyst becomes too strong, the cyst might burst. Water retention due to the SYNDROME, a blow against the abdomen, a fall or accident, exploratory puncture, or premature surgery can cause the rupture. When the cyst breaks, the fluid passes into the abdominal cavity with the released ovarian cells attaching to the abdominal wall (peritoneum) or an abdominal organ such as the bladder or rectum. In this case, the cyst development takes place outside the ovary. This is what is erroneously termed endometriosis. A cyst that forms within an ovary (“deep ovarian endometriosis”) is also called an ovarian endometrioma. If such a cyst contains old menstrual blood, this is referred to as a “chocolate cyst” due to the brown, tar-like color of the fluid-filled cyst cavity.
According to conventional medicine, endometriosis is a “growth of endometrial tissue outside of the uterus”. However, Dr. Hamer's brain scan analyses demonstrate that every woman with endometriosis shows the Hamer Focus, not in the brainstem from where the endometrium (inner lining of the uterus) is controlled but rather in the cerebral medulla, namely in the area of the brain that controls the ovaries (see CT scan above). This also explains why endometriosis increases a woman’s estrogen level, a fact that so far could not have been explained.

Dr. Hamer strongly advises that an ovarian cyst should only be removed when the cyst is fully matured (indurated). Surgery on a semi-liquid cyst disseminates the ovarian cells into the abdominal area causing unnecessary complications. In conventional medicine, the “spreading tumor cells” are usually interpreted as “metastasis”. Moreover, the announcement of the surgery and the actual operation might trigger an “attack conflict” resulting in the development of a peritoneal mesothelioma, a tumor on the abdominal wall at the site of the surgery. The fear of cancer and hospitalization can provoke an existence conflict, leading to the development of ascites (water retention in the abdomen), which is often seen in women after a diagnosis with ovarian cancer.
NOTE: The removal of the ovaries, habitually performed with a hysterectomy (extirpation of the uterus), drastically changes a woman’s hormone status and subsequently her biological identity (see gender, laterality, and hormone status). The amount of estrogen produced in the adrenal glands is not sufficient to compensate for the loss of estrogen production in the ovaries.
|
Are Hysterectomies too common?
“More than 600,000 American women this year will undergo a hysterectomy, or removal of the uterus. That rate is among the highest in the industrialized world. By age 60, one in three women in the U.S. will have had the surgery, and in more cases than not, they will also have had their ovaries and fallopian tubes removed during the procedure. Doctors have long turned to hysterectomy as a treatment for conditions that range from heavy periods to ovarian cancer, but its widespread use concerns some critics who say it's tantamount to female castration.”
TIME, July 17, 2007
|
OVARIES
|

DEVELOPMENT AND FUNCTION OF THE CERVIX UTERI: The cervix uteri or “neck of the uterus” is the lower portion of the uterus that leads into the vaginal canal. The orifice of the cervix opens into the top end of the vagina allowing sperm and menstrual fluid to move through. The cervix is surrounded by a cylinder-shaped muscular structure, the orifice by a sphincter muscle. The inner lining of the cervix uteri is a mucous membrane that secretes fluids, mainly water, to keep the cervical canal moist. The cervix mucosa consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
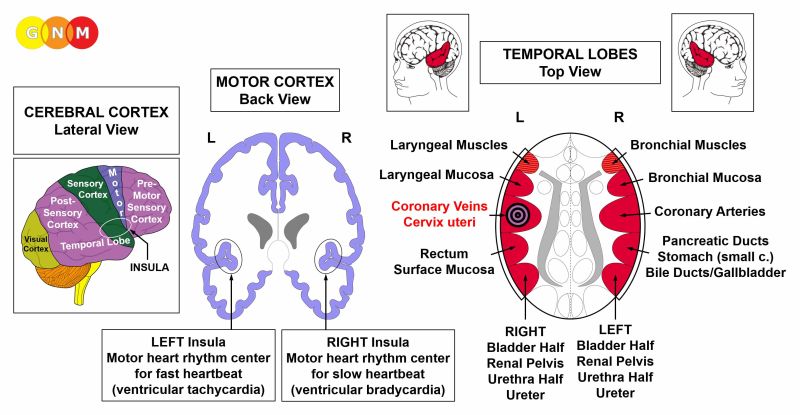
BRAIN LEVEL: The cervix uteri is controlled from the left insula (part of the temporal lobe). The insula is located deep in the cerebral cortex, exactly at the point where the four cerebral cortices meet (pre-motor sensory cortex, motor cortex, sensory cortex, post-sensory cortex).
NOTE: The cervix uteri and the coronary veins share the same brain relay and therefore the same biological conflict. Hence, in females, the Biological Special Programs run simultaneously.
BIOLOGICAL CONFLICT: The biological conflict linked to the cervix uteri is a sexual conflict or mating conflict (meaning, in biological terms, that reproduction is at stake) or a territorial loss conflict, depending on a person’s gender, laterality, and hormone status (see also Postmortal Constellation, Casanova Constellation, Nympho Constellation). In comparison, the conflict associated with the uterus is foremost about “implantation”. In males, the sexual conflict corresponds to the coronary veins (with a low testosterone status) or to the prostate (when the testosterone level is in the normal range).
NHS = Normal hormone status
LES = Low estrogen status
*With left-handers the conflict is transferred to the other brain hemisphere
|
In line with evolutionary reasoning, territorial conflicts, sexual conflicts, and separation conflicts are the primary conflict themes associated with organs of ectodermal origin, controlled from the sensory, pre-motor sensory and post-sensory cortex.
|
A sexual conflict refers to any distress concerning sexuality. This includes painful (first-time) sex, sexual abuse, sexual harassment, unwanted sexual practices, sexual rejection, feeling sexually unwanted, a lack of sexual activity because of an unexpected separation or loss of a mate. Offensive pornography, finding out that the partner or spouse is sleeping with someone else, or interruptions during sexual intercourse can trigger the conflict. As a result of early sexualization, girls experience nowadays the conflict at a very young age. Tubal ligation (“tied tubes”), the use of an IUD, or taking contraceptives to prevent a pregnancy might invoke a sexual conflict on a subtle psycho-biological level.
NOTE: If a woman has a low estrogen status, for example after menopause, she is no longer able to experience a mating conflict in biological terms. She will, therefore, respond to sexual distress more likely with the uterus. This explains, why according to epidemiological studies, 90% of women with uterus cancer are over 50 years of age (Source: Annals of Oncology, 16-41, 2016).
|
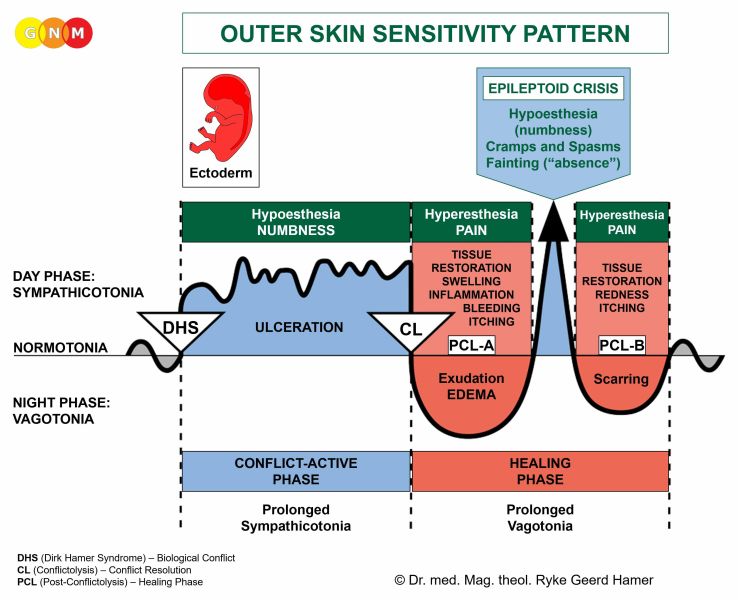 The Biological Special Program of the cervix uteri follows the OUTER SKIN SENSITIVITY PATTERN with hyposensitivity during the conflict-active phase and the Epileptoid Crisis and hypersensitivity in the healing phase.
|
CONFLICT-ACTIVE PHASE: ulceration in the cervix uteri mucosa proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the cervix, so when mating takes place more sperm can reach the uterus which enhances the chance of conception. The conflict affects at the same time the coronary veins. The ulceration of the coronary veins intima causes moderate angina pectoris.

This CT scan shows a Hamer Focus in the area of the brain that controls the cervix uteri (view the GNM diagram). The sharply defined border indicates that the woman is active with a sexual conflict.
With the impact of the conflict in the left temporal lobe (female conflict area) the estrogen level decreases. In GNM, we speak in this case of a conflict-related hormonal imbalance. Depending on the intensity of the conflict, lasting conflict activity results in irregular periods, a delayed menarche (first menstruation), amenorrhea (absence of menstruation), or infertility until the conflict is resolved (see also ovaries).
THE MENSTRUAL CYCLE
in the context of the Five Biological Laws
 Like a Biological Special Program that is initiated by a DHS, the female menstrual cycle has two phases: the follicular phase followed by the luteal phase.
The follicular phase is named for the follicles found in the ovaries. Activated by the follicle stimulating hormone (FSH) secreted by the pituitary gland, between 8 and 15 follicles develop during each menstrual cycle. Only one follicle, however, reaches maturity. It takes 13 days for the follicle to fully mature. The mature follicle contains the egg (ovum) that is ready to be fertilized.
The ovarian follicles produce increasing amounts of estrogen. Hence, during the follicular phase, the estrogen level rises. Estrogen causes the inner lining of the uterus to grow (in accordance with the principle of brainstem and cerebellum controlled organs that generate cell proliferation during the conflict-active phase). The biological purpose of the additional tissue is to thicken the uterus lining to provide an optimum environment for an embryo. This shows that Nature anticipates the fertilization of the egg. The estrogen level reaches its peaks during ovulation.
Ovulation occurs on the 14th day of the menstrual cycle. During ovulation, the mature egg is released from an ovary and swept into one of the two fallopian tubes for fertilization. NOTE: Ovulation is controlled from the left temporal lobe, precisely, from the brain relay that controls the cervix uteri (view the GNM diagram).
A fertilized egg begins immediately the process of embryogenesis, that is, its embryonic development. The developing embryo takes about three days to reach the uterus and another three days to implant into the uterus wall (endometrium). At the time of implantation, the embryo has reached the stage of a blastocyst. Within two weeks, the blastocyst divides into three embryonic germ layers (endoderm, mesoderm, ectoderm) from which all organs and tissues of the human organism develop.
The luteal phase is named for the corpus luteum (“yellow body”) that consists of the cells in the ovarian follicle that are left behind after ovulation. The corpus luteum produces progesterone, a hormone that prepares the uterus for pregnancy. During the first half of the luteal phase the progesterone level rises (the estrogen level drops abruptly after ovulation). If the egg has been fertilized, the corpus luteum continues to secrete progesterone to maintain the new pregnancy. Around the tenth week of pregnancy, the corpus luteum breaks down and the placenta takes over the progesterone production. Progesterone is a hormone that suppresses the production of estrogen. Thus, when a woman is pregnant she is, biologically speaking, a male (progesterone in contraceptives has the same effect). Without fertilization, seven days after ovulation, the corpous luteum disintegrates and the progesterone level decreases. The falling level of progesterone marks the beginning of the premenstrual phase that lasts about seven days. During menstruation the lining of the uterus is shed through the vagina.
The onset of the menstruation is an indication that the female has not become pregnant. In Nature, this is equal to a biological conflict (DHS) that initiates a new menstrual cycle, starting with the follicular phase (conflict-active phase). The ovulation, when the mature egg is released from the follicle and ready for fertilization, is equal to the conflict resolution (CL), followed by the luteal phase (PCL-phase). The premenstrual phase is like a pre-epileptoid phase. Hence, throughout that phase the woman becomes increasingly sympathicotonic. PMS symptoms such as feeling nervous and irritable occur during this period of the luteal phase. The menstruation with abdominal cramps caused by the contraction of the uterus muscles is similar to an Epileptoid Crisis.
|
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss in the cervix uteri is replenished through cell proliferation with swelling due to the edema (fluid accumulation) in the healing area. In conventional medicine, a profuse cell proliferation is diagnosed as a cervical cancer. Based on the Five Biological Laws, the new cells cannot be regarded as “cancer cells” since the cell increase is, in reality, a replenishing process.
Healing symptoms are pain and bleeding from the cervix, ranging from mild to severe. There might also be some yellow discharge due to bacterial activity. A prolonged, intense healing process (hanging healing) causes long and heavy menstrual periods (see also uterus mucosa, uterus muscles, ovaries, and manic depression). Throughout the Epileptoid Crisis, the muscles in the inner wall of the cervical canal contract with painful cramps. Other symptoms of the Epi-Crisis are a rapid heartbeat (tachycardia) since the coronary veins undergo the healing crisis at the same time.
NOTE: All Epileptoid Crises that are controlled from the sensory, post-sensory, or pre-motor sensory cortex are accompanied by troubled circulation, dizzy spells, short disturbances of consciousness or a complete loss of consciousness (fainting or “absence”), depending on the intensity of the conflict. Another distinctive symptom is a drop of blood sugar caused by the excessive use of glucose by the brain cells (compare with hypoglycemia related to the islet cells of the pancreas).
|
In PCL-B, the swelling in the cervix slowly subsides; so does the bleeding and the pain. Cervical warts, also called genital warts or condyloma, are the result of continuous conflict relapses (see also vaginal warts).

The PAP TEST is a cancer screening test that checks for changes in the cervical tissue. Hence, the test can be positive (“pre-cancerous”) in the conflict-active phase (ulceration in the cervic uteri mucosa) as well as in the healing phase (restoration of the squamous epithelial layer of the cervix uteri through cell proliferation). None of these changes are “abnormal” but occur naturally during the two phases of the Biological Special Program. As the PSA test, a Pap test is just a marker indicating the degree of conflict activity or healing.
The medical industry claims that cervical cancer is caused by the so-called Human Papilloma Virus (HPV), allegedly transmitted through sexual contact. In 2006, the FDA approved the vaccine Gardasil to supposedly “protect” teen girls against “cervical cancer”. The vaccine is also imposed on boys at the ages of 9 to 12 to “prevent the spread of the HPV infection”.
“The cervical cancer risk in the U.S. is already extremely low, and vaccinations are unlikely to have any effect upon the rate of cervical cancer in the United States. In fact, 70% of all HPV infections resolve themselves without treatment in a year, and the number rises to well over 90% in two years” (Diane Harper).
Dr. Diane Harper was a leading expert responsible for the Phase II and Phase III safety and effectiveness studies which secured the approval of the human papilloma virus (HPV) vaccines, Gardasil™ and Cervarix™. She is now the latest in a long string of experts who are pressing the red alert button on the devastating consequences and irrelevancy of these vaccines. Dr. Harper made her surprising confession at the 4th International Conference on Vaccination which took place in Reston, Virginia, in 2015.
Source: C. Thomas Corriher, Defy your doctor and be healed, 2013
|
 a HPV has never been isolated and scientifically proven.”
T. Engelbrecht and C. Koehnlein, Virus Mania, 2007
|
CERVIX UTERI
|

DEVELOPMENT AND FUNCTION OF THE CERVICAL MUSCLES AND CERVICAL SPHINCTER: The cervix uteri is surrounded by a body of muscles with a sphincter muscle at the opening into the vagina. During labor, the cervical muscles contract and the sphincter opens to aid the delivery of the child (see also uterus muscles and vaginal muscles). The same occurs during the female orgasm where the cervical sphincter relaxes so that the penis can penetrate easily into the cervix with the cervical muscles holding the penis tight. The cervical muscles and the cervical sphincter are composed of striated muscles, originate from the new mesoderm and are controlled from the cerebral medulla and the motor cortex.

BRAIN LEVEL: The cervical muscles and cervical sphincter have two control centers in the cerebrum. The trophic function of the muscles, responsible for the nutrition of the tissue, is controlled from the cerebral medulla; the contraction of the muscles is controlled from the motor cortex (part of the cerebral cortex). The right half of the cervical muscles and cervical sphincter are controlled from the left side of the cerebrum; the left halves are controlled from the right cerebral hemisphere. Hence, there is a cross-over correlation from the brain to the organ (see GNM diagram showing the motor homunculus).
NOTE: The cervical muscles and cervical sphincter, vaginal muscles, bladder muscle and external bladder sphincter, rectal muscles and external anal sphincter share the same brain relays.
BIOLOGICAL CONFLICT: The biological conflict linked to the cervical muscles and cervical sphincter is “not being able to sufficiently hold the fetus” (difficult pregnancy, fear of miscarriage, abortions; see also uterus muscles) or “not being able to hold the penis tight enough during intercourse” (compare with vaginal muscles). The conflict is similar to a self-devaluation conflict.
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of cervical muscle tissue (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing paralysis or weakness of the cervical muscles (controlled from the motor cortex). At the same time, the cervical sphincter opens (no necrosis with sphincters!).
NOTE: The striated muscles belong to the group of organs that respond to the related conflict with functional loss (see also Biological Special Programs of the islet cells of the pancreas (alpha islet cells and beta islet cells), inner ear (cochlea and vestibular organ), olfactory nerves, retina and vitreous body of the eyes) or hyperfunction (periosteum and thalamus).
|
NOTE: External sphincters (external bladder sphincter, external anal sphincter, cervical sphincter) consist of striated muscles, while internal sphincters such as the internal bladder sphincter and internal anal sphincter consist of smooth muscles. External sphincters have an inverse innervation, meaning that they close through contraction in vagotonia, i.e., in the healing phase, and open through relaxation in sympathicotonia, i.e., in the conflict-active phase and Epileptoid Crisis. Regarding the cervical sphincter, sudden distress suffered by a pregnant woman or by the unborn opens the sphincter inducing a premature birth or miscarriage.
|
HEALING PHASE: During the healing phase, the cervical muscles are reconstructed and the cervical sphincter closes. The Epileptoid Crisis presents as cervical spasms.
NOTE: All organs that derive from the new mesoderm (“surplus group”), including the cervical muscles, show the biological purpose at the end of the healing phase. After the healing process has been completed, the organ or tissue is stronger than before, which allows being better prepared for a conflict of the same kind.
|
 THE FEMALE ORGASM
During the female orgasm, the cervical sphincter opens while the cervical muscles contract (equal to the rhythmic muscle contraction that occurs in the Epileptoid Crisis of the skeletal muscles). When the male ejaculates, the “sucking” movement of the cervix helps to draw the semen into the uterus. The cervical (rather than vaginal) orgasm is initiated from the “female conflict area” on the left side of the cerebral cortex, precisely, from the brain relay that controls the cervix uteri. At the height of the orgasm, the entire left temporal lobe becomes involved, including the larynx (gasping) and the rectum. Both the clitoral orgasm and penile orgasm are controlled from the right side of the post-sensory cortex (see clitoris); the rectal orgasm is controlled from the left side.
|

DEVELOPMENT AND FUNCTION OF THE BARTHOLIN’S GLANDS: The Bartholin’s glands are located on each side of the opening to the vagina. Equal to the smegma producing glands that lubricate the penis head, the function of the Bartholin’s glands is to secrete mucus (secretory quality) to lubricate the vaginal entrance in preparation for sexual intercourse. The Bartholin’s glands consist of intestinal cylinder epithelium, originate from the endoderm and are therefore controlled from the brainstem.
NOTE: The Skene’s gland, situated on the upper wall of the vagina, is the equivalent to the male prostate gland. The secretions produced by the Skene’s gland contain prostatic fluid, including PSA! As with the prostate, the ducts of the gland open into the urethra. During sexual arousal, the fluid is expelled through the urethral opening, explaining “female ejaculation”. In 2002, the Federative International Committee on Anatomical Terminology officially renamed the Skene's gland to “female prostate”.
|

BRAIN LEVEL: The Bartholin’s glands are controlled from the left side of the brainstem. The control center is located next to the control center of the rectum submucosa.
NOTE: The Bartholin’s glands, smegma producing glands, and bladder submucosa (bladder trigone) share the same brain relay.
BIOLOGICAL CONFLICT: The biological conflict linked to the Bartholin’s glands is “not being able to produce sufficient vaginal mucus”. Insufficient foreplay and painful sex when the vagina is not lubricated enough typically activate the conflict.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the Bartholin’s glands proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to augment the secretion of vaginal mucus to facilitate easier penetration.
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer required. If the healing process is intense, the accumulation of pus forms an abscess (Bartholin’s abscess) or a fluid-filled cyst (Bartholin’s cyst) that empty spontaneously during the Epileptoid Crisis. With concurrent water retention due to the SYNDROME, the abscess or cyst might occlude the duct exiting the gland.
When fungi assist healing, this causes candidiasis (see also candidiasis related to the uterus mucosa and fallopian tubes). The fungal discharge produced during the cell removal is excreted through the vaginal opening. NOTE: The “vaginal discharge” originates in the Bartholin’s glands and not, as assumed, in the vagina since the vaginal canal is not endowed with an endodermal submucosa and subsequently not populated by fungi or TB bacteria. Frequent conflict relapses lead to a loss of glandular tissue resulting in permanent vaginal dryness (see also vaginal mucosa). Like other so-called venereal diseases, candidiasis is not contagious! If the male partner happens to have the condition as well, this reveals that he experienced – at the same time – the conflict of “not being able to penetrate a tight or dry vagina” with subsequent penile candidiasis in the healing phase.
NOTE: Antibiotics also cause vaginal dryness. They destroy the normal vaginal flora that is largely inhabited by Lactobacillus acidophilus bacteria. The “fungal infection” is brought on by the side-effects of the medication (“not being able to produce sufficient vaginal mucus”). The candidiasis symptoms (discharge, itching) occur in the healing phase or after the antibiotic treatment is over. Further treatments create a vicious cycle.
|

DEVELOPMENT AND FUNCTION OF THE VAGINAL MUCOSA: The vagina is the passageway that leads from the cervix uteri to the exterior of the body. The outside wall of the vagina is composed of muscles. The interior surface is a layer of connective tissue allowing for greater elasticity during sexual intercourse and childbirth. The mucous membrane of the inner lining maintains a steady level of moisture in the vaginal canal. The vagina itself has no glands. However, blood plasma seeping through the permeable vaginal walls keeps the vagina moist at all times. When a woman becomes sexually aroused, the increased blood flow to the area causes more fluid to seep through. The Bartholin’s glands produce mucus at the opening of the vagina to facilitate the penetration of the penis. The vaginal mucosa consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex. NOTE: The vagina does not have an endodermal submucosa.

BRAIN LEVEL: The vaginal mucosa is controlled from the sensory cortex (part of the cerebral cortex). The right half of the vagina is controlled from the left side of the sensory cortex; the left half is controlled from the right cortical hemisphere. Hence, there is a cross-over correlation from the brain to the organ (see GNM diagram showing the sensory homunculus).
NOTE: The vaginal mucosa and epidermis of the external genitals (male and female) share the same brain relays (see GNM diagram).
BIOLOGICAL CONFLICT: The biological conflict linked to the vaginal mucosa is a sexual separation conflict associated with the vagina. Similar to a sexual conflict related to the cervix uteri, a woman can suffer the conflict through the unexpected loss of a sexual mate, sexual rejection, her partner’s impotence, or when she finds out that her man is sleeping with someone else. The suspicion that her partner has sexual contact with another female can already trigger the conflict. Conversely, a sexual separation conflict refers to not wanting to have sex, for example, because of a lack of emotional intimacy, painful intercourse, insufficient foreplay, unwanted sexual practices, or a fear of getting pregnant. The fear of contracting a venereal disease can also provoke the conflict.
In line with evolutionary reasoning, territorial conflicts, sexual conflicts, and separation conflicts are the primary conflict themes associated with organs of ectodermal origin, controlled from the sensory, pre-motor sensory and post-sensory cortex.
|
The Biological Special Program of the vaginal mucosa follows the OUTER SKIN SENSITIVITY PATTERN with hyposensitivity during the conflict-active phase and the Epileptoid Crisis and hypersensitivity in the healing phase.
|
CONFLICT-ACTIVE PHASE: ulceration (cell loss) in the vaginal mucosa with a decrease or, with intense conflict activity, a complete loss of sensitivity. The vaginal hyposensitivity (numbness) serves the biological purpose of not being able to “feel” anything in order to be better able to cope with the sexual separation (see short-term memory loss with a separation conflict).
Ongoing ulceration in the vagina leads to vaginal dryness (see also Bartholin’s glands). For women who are sexually active, the pain during intercourse causes usually new sexual separation conflicts together with the distress of “not being able to produce sufficient vaginal mucus”. As a result, the vaginal dryness becomes chronic.
NOTE: Vaginal lubrication is controlled from the parasympathetic nervous system. This is why the vagina does not become moist when a woman is under stress or with intense conflict activity (sympathicotonia) of any biological conflict (the same applies to the penile erection).
|
HEALING PHASE: During the first part of the healing phase (PCL-A) the ulceration is replenished through cell proliferation. Healing symptoms are vaginal dermatitis with vaginal itching (pruritus) and pain (hypersensitivity). With an inflammation, the condition is called vaginitis. The vaginal discharge is clear, potentially with some light bleeding; when bacteria assist healing, the discharge is yellow (compare with discharge produced through fungal activity in the uterus or Bartholin’s glands).
After the Epileptoid Crisis, in PCL-B, the condition normalizes, provided there are no conflict relapses.
NOTE: All Epileptoid Crises that are controlled from the sensory, post-sensory, or pre-motor sensory cortex are accompanied by troubled circulation, dizzy spells, short disturbances of consciousness or a complete loss of consciousness (fainting or “absence”), depending on the intensity of the conflict. Another distinctive symptom is a drop of blood sugar caused by the excessive use of glucose by the brain cells (compare with hypoglycemia related to the islet cells of the pancreas).
|
Vaginal herpes are blisters and sores in the vagina. According to conventional medicine, genital herpes is a “sexually transmitted disease” caused by a “herpes virus”, a theory that has never been scientifically proven. Like other venereal diseases, genital herpes cannot be sexually transmitted since the symptoms are already healing symptoms.
Vaginal warts, also called genital warts or condyloma, are the result of continuous conflict relapses (see also cervical warts).

DEVELOPMENT AND FUNCTION OF THE VAGINAL MUSCLES: The vaginal muscles surround the entire vaginal canal. Their function is to hold the penis during sexual intercourse and to expand and contract throughout labor to facilitate delivery (see also cervical muscles, cervical sphincter and uterus muscles). The vaginal muscles are striated muscles, derive therefore from the new mesoderm and are controlled from the cerebral medulla and the motor cortex.

BRAIN LEVEL: The vaginal muscles have two control centers in the cerebrum. The trophic function of the muscles, responsible for the nutrition of the tissue, is controlled from the cerebral medulla; the contraction and expansion of the muscles are controlled from the motor cortex (part of the cerebral cortex). The right half of the vaginal musculature is controlled from the left side of the cerebrum; the left half is controlled from the right cerebral hemisphere. Hence, there is a cross-over correlation from the brain to the organ (see GNM diagram showing the motor homunculus).
NOTE: The vaginal muscles, cervical muscles and cervical sphincter, bladder muscle and external bladder sphincter, rectal muscles and external anal sphincter share the same brain relays.
BIOLOGICAL CONFLICT: The biological conflict linked to the vaginal muscles is “not being able to hold the penis” or not being able to prevent vaginal penetration (forced sex, unwanted sex, a fear of sexual intercourse because of discomfort or pain).
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of vaginal muscle tissue (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing weakness of the vaginal muscles (controlled from the motor cortex), which is usually not noticed.
NOTE: The striated muscles belong to the group of organs that respond to the related conflict with functional loss (see also Biological Special Programs of the islet cells of the pancreas (alpha islet cells and beta islet cells), inner ear (cochlea and vestibular organ), olfactory nerves, retina and vitreous body of the eyes) or hyperfunction (periosteum and thalamus).
|
HEALING PHASE: In the healing phase the vaginal muscles are reconstructed. However, during the Epileptoid Crisis the muscles contract causing tonic-clonic vaginal cramps, a condition known as vaginismus. The distress associated with painful intercourse can become a track resulting in symptom relapses.
NOTE: All organs that derive from the new mesoderm (“surplus group”), including the vaginal muscles, show the biological purpose at the end of the healing phase. After the healing process has been completed, the organ or tissue is stronger than before, which allows being better prepared for a conflict of the same kind.
|

DEVELOPMENT AND FUNCTION OF THE GLANS CLITORIS: The clitoris is situated within the front junction of the inner labia, above the opening of the urethra. The clitoris is made up of the glans, the clitoral shaft, and the clitoral hood. The clitoral glans consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex. NOTE: The clitoral glans is covered by an epidermal skin layer but not endowed with a corium skin (under skin).

The clitoral shaft is equivalent to the penile corpora cavernosa that extend from the lower branches of the pubic bone to the penis head. In females, the two cavernous bodies are located underneath the outer labia. The crura are projections of the corpora cavernosa. Like the corpus spongiosum of the penis, the vestibular bulbs of the clitoris are erectile tissue composed mainly of smooth muscles.

BRAIN LEVEL: The glans clitoris is controlled from the post-sensory cortex (part of the cerebral cortex). The epidermis covering the glans is controlled from the sensory cortex (see brain relays of external genitals and vaginal mucosa).
The right half of the glans clitoris is controlled from the left side of the post-sensory cortex (between the rectum and right bladder relays); the left half is controlled from the right cortical hemisphere (between the stomach and left bladder relays). Hence, there is a cross-over correlation from the brain to the organ.
NOTE: The glans clitoris and glans penis share the same brain relays. Their control centers are located outside of the temporal lobes; hence, the principle of gender, laterality, and hormone status does not apply.
BIOLOGICAL CONFLICT: The biological conflict linked to the glans clitoris is a severe separation conflict associated with the clitoris, for example, through the loss of a sexual mate or sexual rejection (see also sexual separation conflict related to the vagina and to the epidermis of the external genitals). The conflict also refers to not wanting to be touched at the clitoris (sexual abuse, sexual molestation, resistance to oral sex, unpleasant clitoral stimulation) or not being allowed to be touched at the clitoris, including touching oneself (a DHS triggered when caught masturbating).
In line with evolutionary reasoning, territorial conflicts, sexual conflicts, and separation conflicts are the primary conflict themes associated with organs of ectodermal origin, controlled from the sensory, pre-motor sensory and post-sensory cortex.
|
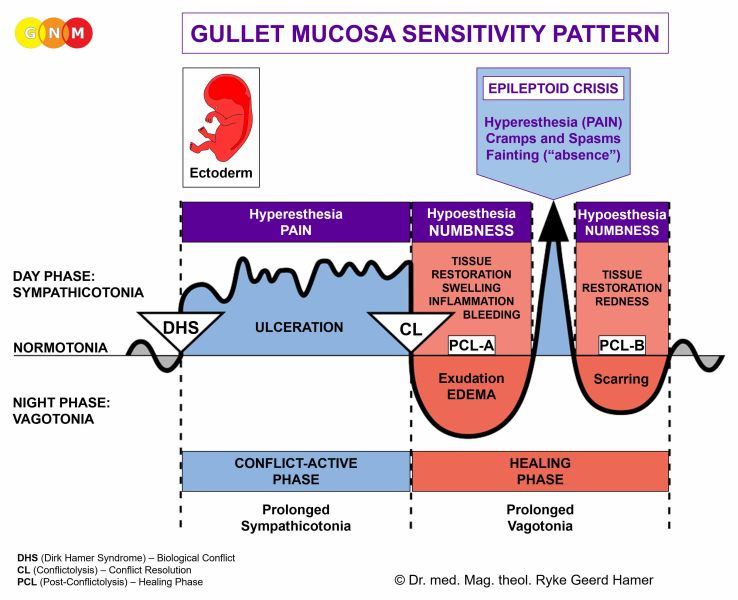 The Biological Special Program of the glans clitoris follows the GULLET MUCOSA SENSITIVITY PATTERN with hypersensitivity during the conflict-active phase and the Epileptoid Crisis and hyposensitivity in the healing phase.
NOTE: With the exception of the glans penis and glans clitoris, the external genitals follow the Outer Skin Sensitivity Pattern since they are controlled from the sensory cortex.
|
CONFLICT-ACTIVE PHASE: ulceration (cell loss). During conflict activity, the clitoral glans is overly sensitive to touch (hypersensitivity).
HEALING PHASE: During the healing phase the ulceration is replenished with new cells. The healing process manifests as clitoral hyposensitivity (numbness) with decreased or, if the conflict was intense, a complete loss of sensitivity. The hypersensitivity is briefly reactivated during the Epileptoid Crisis. With the completion of the Biological Special Program, the clitoral sensitivity returns to normal.
NOTE: All Epileptoid Crises that are controlled from the sensory, post-sensory, or pre-motor sensory cortex are accompanied by troubled circulation, dizzy spells, short disturbances of consciousness or a complete loss of consciousness (fainting or “absence”), depending on the intensity of the conflict. Another distinctive symptom is a drop of blood sugar caused by the excessive use of glucose by the brain cells (compare with hypoglycemia related to the islet cells of the pancreas).
|
FEMALE SEXUAL ORGANS - TRANSLATIONS
| ||||||||||