Liver and Gallbladder
 DEVELOPMENT AND FUNCTION OF THE LIVER PARENCHYMA: The liver parenchyma forms the bulk of the liver. It consists for the most part of so-called hepatocytes, which are the prime functional cells of the liver. Their main activities are the production of bile (secretory quality), a substance that helps to remove toxins from the body. Bile made in the liver travels via the common bile duct to the small intestine where it aids the absorption of fats (absorptive quality). During times, when bile is not needed in the intestines, it is stored in the gallbladder until required. In addition to secreting bile, the liver also produces cholesterol. The liver parenchyma is composed of intestinal cylinder epithelium, originates from the endoderm and is therefore controlled from the brainstem.
 BRAIN LEVEL: In the brainstem, the control center of the liver parenchyma is orderly positioned within the ring form of the brain relays that control the organs of the alimentary canal, precisely, on the right brainstem hemisphere between the stomach and the pancreas relays.
BIOLOGICAL CONFLICT: The biological conflict linked to the liver parenchyma is a starvation conflict.
A person can suffer a starvation conflict in real terms due to a lack of food. Hence, being put on a strict diet, not being allowed to eat one’s favorite food, a colon cancer diagnosis associated with not getting food through the intestine, wearing a colostomy bag, ongoing diarrhea, a loss of appetite and excessive vomiting during chemo treatments, or unintentional weight loss might trigger the conflict. However, a “threat of starvation” could also be brought on when one is – unexpectedly – in a situation of not being able to make ends meet, let’s say, because of the loss of a workplace, pay cuts, the loss of a business, bankruptcy, the loss of clients, an unexpected rent increase, an economically devastating divorce, the confiscation of property, the loss of savings, financial debts, or losing a family member who provided financial support. In short, the conflict translates into the distress of running out of resources to feed oneself and those one feels responsible for.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase liver cells (hepatocytes) proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to improve the function of the liver so that the smallest food particles can be used to its optimum. With prolonged conflict activity (hanging conflict) liver nodules, referred to as a liver cancer (“hepatocellular carcinoma”), develop as a result of the continuing cell augmentation (compare with “liver cancer” related to the bile ducts). Usually, the nodules are flat-growing (absorptive type); infrequently, they take a cauliflower-like shape (secretory type). If the rate of cell division exceeds a certain limit, conventional medicine considers the cancer as “malignant”. “Benign” liver nodules are termed Focal Nodular Hyperplasia (FNH).
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer required. Healing symptoms are pain due to the swelling of the liver and night sweats. The liver blood parameters are in the normal range. A liver abscess is a liver nodule filled with pus. What is commonly called a “fatty liver” refers, in GNM terms, to fat deposits in the healing liver.
Liver tuberculosis, indicating the activity of TB bacteria, is much more frequent in regions where there is famine, such as in Africa (see also kidney tuberculosis linked to an existence conflict and lung tuberculosis related to a death-fright conflict). The correlation between tuberculosis and poverty has long been noticed by medical historians. In the Western world, where tuberculosis is supposed to be eradicated, liver tuberculosis is now called liver cancer (see also renaming of lung tuberculosis to lung cancer and kidney tuberculosis to “nephrotic syndrome”). The disease names have changed, the symptoms didn’t!
 On this brain CT, we see two brain edemas in the area of the brainstem that controls the liver parenchyma (view the GNM diagram), revealing that the person is in the healing phase (PCL-A) of two independent starvation conflicts.
 On an organ CT, the liver nodules appear as round dark spots.
The liver is the only organ that is capable of regenerating itself by making new liver tissue (Prometheus phenomenon). However, when healing is prolonged (hanging healing) and continually interrupted by conflict relapses, the ongoing decomposing process leaves caverns in the liver (see also pancreas caverns, lung caverns, breast gland caverns). Liver cysts (also called “polycystic liver disease”) develop when the caverns are filled with water due to an active abandonment or existence conflict (the SYNDROME).
Water retained in the healing liver leads to an enlarged liver or hepatomegaly (see also hepatomegaly related to the bile ducts), often with an ascites caused by the excess water in the peritoneum. A large swelling close to the common hepatic duct bears the risk of a mechanical obstruction of the bile duct with symptoms characteristic for jaundice. Acute complications arise when the swelling compresses the portal vein. In this case, surgery is a must.
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the liver nodules cannot be broken down and therefore remain. Eventually, they become encapsulated with connective tissue. Such “tumors” are often accidentally discovered during a routine checkup or follow-up examination. Hence, today’s excessive use of antibiotics contributes significantly to the increasing number of cancers that are detected during medical exams.
|
 DEVELOPMENT AND FUNCTION OF THE BILE DUCTS: The bile ducts branch through the liver in a tree-like structure. The common hepatic duct joins the cystic duct coming from the gallbladder to form the common bile duct. The common bile duct meets the pancreatic duct before it opens into the intestine. Bile, produced in the liver and stored in the gallbladder, flows into the duodenum (the first section of the small intestine) where it is required for the digestion of food, particularly of fats. Bile also helps the body get rid of waste material that is filtered out of the bloodstream by the liver. The lining of the bile ducts consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
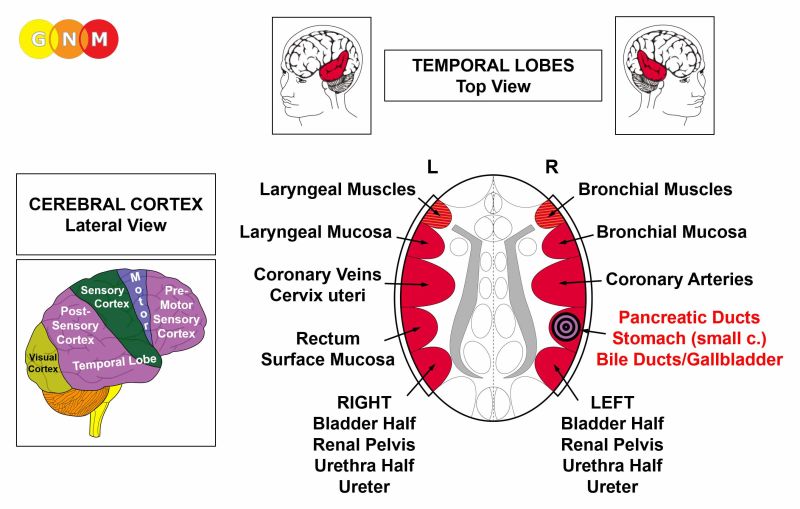 BRAIN LEVEL: The epithelial lining of the bile ducts is controlled from the right temporal lobe (part of the post-sensory cortex). The control center is positioned exactly across from the brain relay for the rectum lining.
NOTE: The bile ducts, gallbladder, stomach (small curvature), pylorus, duodenal bulb, and pancreatic ducts share the same brain relay and therefore the same biological conflict. Which one of these organs will be affected by the DHS is random. A severe conflict can affect all organs at once.
BIOLOGICAL CONFLICT: The biological conflict linked to the bile ducts is a male territorial anger conflict (fight in the territory) or a female identity conflict, depending on a person’s gender, laterality, and hormone status (see also Aggressive Constellation).
A territorial anger relates to anger in the environment and places which one considers as his or her domain – literally or figuratively. Typical territorial anger conflicts are disputes at home, feuds at the workplace, anger at school, in kindergarten, at the playground, in a seniors or nursing home, or in the hospital; also in the extended “territory” such as in the village, town, or country where one lives. Battles over a land or property, annoying noise in the house or neighborhood, a fight over a parking place or over a toy, are other examples of what can provoke a territorial anger conflict.
CONFLICT-ACTIVE PHASE: ulceration in the lining of the bile ducts proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the ducts to enhance the flow of bile to the intestine for better digestion. This, in turn, improves the metabolism providing the individual with more energy to resolve the conflict. Depending on the intensity of the territorial anger conflict, the ulceration affects one or several ducts. The symptom: mild to severe pain.
 This brain CT shows the impact of a territorial anger conflict in the bile ducts relay (view the GNM diagram. The mostly sharp border of the Hamer Focus indicates that the person is still conflict active; the edematous parts (dark) point to short healing phases that are interrupted by conflict relapses.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation. In conventional medicine, this is usually diagnosed as a “liver cancer” (compare with liver cancer related to the liver parenchyma). Based on the Five Biological Laws, the new cells cannot be regarded as “cancer cells” since the cell increase is, in reality, a replenishing process.
Healing symptoms are swelling due to the edema (fluid accumulation) and abdominal pain, which could last throughout the entire healing phase (in PCL-A and PCL-B the pain is not of a sensory nature but pressure pain). Concurrent water retention because of the SYNDROME enlarges the swelling and increases the pain.
A large swelling in the common bile duct or in several ducts blocks the bile flow resulting in jaundice. Jaundice shows as yellow skin and a yellow sclera; also, the urine becomes brown and the stool light yellow due to the lack of bilirubin. A pancreas tumor can lead to jaundice when the tumor obstructs the common bile duct that connects the pancreas to the liver. Jaundice is quite common in newborns. Conventional medicine presumes that this is linked to a baby’s still developing liver not being yet able to remove adequate bilirubin from the blood. However, if this were correct, why is then not every baby born with jaundice? From the GNM perspective, jaundice in newborns is rather caused by a territorial anger that occurred already in the womb (see intrauterine conflicts). A fetus can also suffer a territorial anger conflict with or on behalf of the mother. Distress in the delivery room, a difficult delivery, or the way the newborn is handled at birth can evoke a territorial anger with jaundice in the healing phase, when the baby feels safe.
Hepatitis occurs when healing is accompanied by an inflammation. “Acute hepatitis” indicates that the bile duct-related conflict is reactivated through setting on tracks established when the original territorial anger took place. “Chronic hepatitis” reveals a hanging healing due to continual conflict relapses that delay the completion of the healing phase. Icteric hepatitis with the typical symptoms of jaundice develops when a bile duct occlusion involves several ducts or the common hepatic duct.
Conventional medicine claims that hepatitis is caused by hepatitis viruses (A, B, C, D, E). However, as demonstrated in the publication Virus Mania by Torsten Engelbrecht and Claus Köhnlein, “certainly nobody has yet managed to detect a corresponding virus structure in the blood serum of so-called hepatitis C patients. As with HIV, the virus purification necessary for a clear identification has not taken place” (p. 155). In short, none of the alleged hepatitis viruses – or any virus – has ever been scientifically verified (details are presented in the “Virus Mania” GNM video). This seriously questions the justification of vaccinating newborns and of imposing “immunization” on travelers who, naturally, develop hepatitis after having resolved the territorial anger conflict – away from the “anger”-environment.
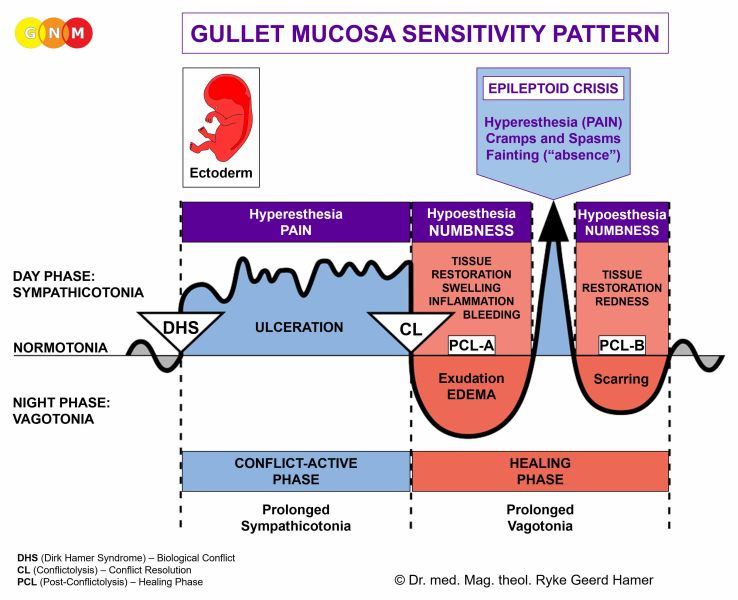
With hepatitis, the level of Gamma-GT, a significant liver enzyme parameter, rises in PCL-A with a sharp drop during the Epileptoid Crisis. The Epileptoid Crisis presents as acute sharp pain and cramps or spasms (liver colic) if the surrounding striated muscles of the bile ducts undergo the Epileptoid Crisis at the same time. In PCL-B, the bile ducts open and the function of the organ returns to normal.
Hepatitis with the SYNDROME, that is, with water retention due to an active abandonment or existence conflict involving the kidney collecting tubules causes an enlargement of the liver (hepatomegaly) with acute pain (see also hepatomegaly related to the liver parenchyma). Excessive water retention could create a critical situation, since the additional water is also stored in the brain edema that develops parallel to the edema on the healing organ. Because of the strong brain pressure a person might fall into a coma (hepatic coma) and die.
Liver cirrhosis is the consequence of constant relapses of territorial anger conflicts. As a result of the recurring repair processes in the bile ducts, the squamous epithelial lining is gradually replaced by scar tissue (in PCL-B). Over time, this severely compromises the function of the liver. Hence, without addressing the underlying conflict, the condition might be fatal. About 50% of patients with liver cirrhosis also develop an ascites (water belly). According to conventional medicine, the fluid in the abdomen is caused by high blood pressure in the portal vein of the liver (the same theory is applied to esophageal varices). If this theory were valid, why does “cirrhotic ascites” then not occur in 100% of the cases? Based on the knowledge of GNM, the water retained in the abdominal cavity indicates that the person is experiencing territorial anger and abandonment or existence conflicts at the same time. An existence conflict could also be caused by the diagnosis shock, since liver cirrhosis has generally a poor prognosis.
Liver cirrhosis has nothing to do with alcohol consumption (just as there is no correlation between smoking and the development of lung cancer). There are people who have liver cirrhosis who don’t drink and there are alcoholics who never develop liver cirrhosis. But territorial anger conflicts and drinking often go together! Dr. Hamer: “The majority of alcoholics belong to the lower classes of society. There, they are much more vulnerable to suffer conflicts than 'good' citizens. Liver cancer does not come from alcohol, but alcohol and cancer come from sorrow and misery.”
|
 DEVELOPMENT AND FUNCTION OF THE GALLBLADDER: The gallbladder connects to the hepatic system with the cystic duct that leads directly into the common bile duct. During periods when bile, made in the liver, is not flowing into the intestine it is diverted into the gallbladder, where it is stored until needed for digestion. The lining of the gallbladder consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
BRAIN LEVEL: The epithelial lining of the gallbladder is controlled from the right temporal lobe (part of the post-sensory cortex). The control center is positioned exactly across from the brain relay of the rectum lining.
NOTE: The gallbladder, bile ducts, stomach (small curvature), pylorus, duodenal bulb, and pancreatic ducts share the same brain relay and therefore the same biological conflict. Which one of these organs will be affected by the DHS is random. A severe conflict can affect all organs at once.
BIOLOGICAL CONFLICT: The biological conflict linked to the gallbladder is a male territorial anger conflict or a female identity conflict, depending on a person’s gender, laterality, and hormone status (see bile ducts).
A territorial anger relates to anger in the environment and places which one considers as his or her domain – literary or figuratively. Typical territorial anger conflicts are disputes at home, feuds at the workplace, anger at school, in kindergarten, at the playground, in a seniors or nursing home, or in the hospital; also in the extended “territory” such as in the village, town, or country where one lives. Battles over a land or property, annoying noise in the house or neighborhood, a fight over a parking place or over a toy, are other examples of what can provoke a territorial anger conflict.
CONFLICT-ACTIVE PHASE: ulceration in the lining of the gallbladder proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to increase the flow of bile to the intestine, which provides the individual with more energy to resolve the conflict. The ulceration could also involve the cystic duct. The symptom: mild to severe pain, depending on the intensity of the territorial anger conflict.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation. Healing symptoms are swelling due to the edema (fluid accumulation) and abdominal pain (in PCL-A and PCL-B the pain is not of a sensory nature but pressure pain). Concurrent water retention due to the SYNDROME enlarges the swelling and increases the pain. With an inflammation the condition is called cholecystitis.
The Epileptoid Crisis manifests as acute pain and cramps or spasms (biliary colic) if the surrounding striated muscles of the gallbladder undergo the Epileptoid Crisis at the same time. The Epi-Crisis could last up to thirty hours. With a hanging healing, that is, when the healing phase is continually interrupted by conflict relapses, the buildup of bile eventually leads to the formation of gallstones. At one point during the Epileptoid Crisis, they are pushed through the cystic duct and the common bile duct into the small intestine, which is very painful. In PCL-B the gallbladder slowly returns to its normal function.
| ||||||||||||||||