Mouth and Pharynx
THE SIX QUALITIES OF THE ALIMENTARY CANAL
 EMBRYONIC GERM LAYER: The organs of the alimentary canal – from the mouth to the rectum – derive from the oldest embryonic germ layer, which is the endoderm, and are therefore controlled from the brainstem, the oldest part of the brain.
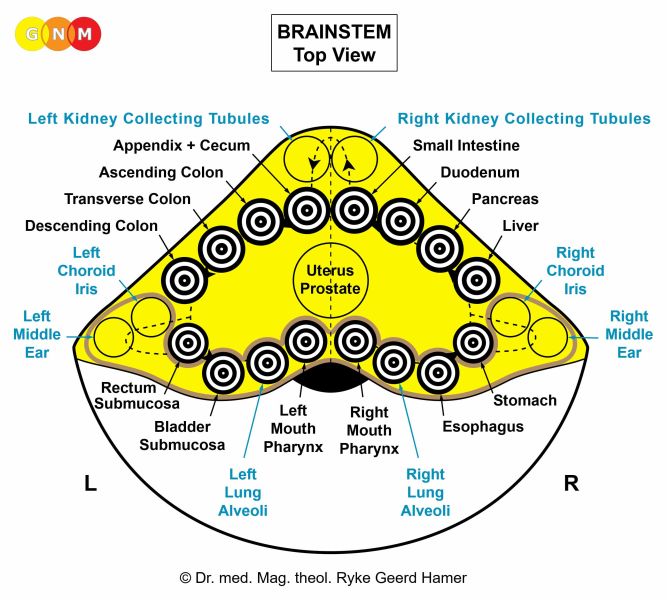 BRAIN LEVEL: In the brainstem, the control centers of the organs of the digestive system and its descendants are positioned in a ring-form order, starting on the right brain hemisphere with the brain relays of the mouth and pharynx (incl. thyroid gland, parathyroid glands), esophagus, stomach, liver parenchyma, pancreas gland, duodenum, small intestine continuing counter-clockwise with the control centers of the appendix, cecum, colon, rectum, and the bladder on the left side of the brainstem.
BIOLOGICAL CONFLICTS: According to their function, the biological conflicts linked to the organs of the alimentary canal are MORSEL CONFLICTS of “not being able to catch/eliminate a morsel” (mouth and pharynx), “not being fast enough to catch/eliminate a morsel” (thyroid gland), “not being able to swallow a morsel” (esophagus), and “not being able to absorb and digest a morsel” (pancreas, stomach, duodenum, small intestine, colon). For animals, a morsel concerns a real piece of food whereas for humans a morsel can also be of a figurative nature.
Sensory quality: relates to analyzing a food morsel according to its chemical make-up, that is, whether the morsel is useful (nutritious) or harmful (poisonous) for the organism. If a disagreeable morsel is in the mouth or pharynx, the instinctive reaction is to spit the morsel out; if an “indigestible morsel” is in the stomach, the vomiting reflex is activated in order to eliminate the morsel; if it has already reached the small intestine, this causes diarrhea.
Excretory quality: relates to the excretion of toxic waste. Toxic substances that cannot be excreted through the kidneys are excreted into the intestine. NOTE: With diarrhea caused by disagreeable food, the sensory, motor, and excretory qualities go together without a cell increase.
|
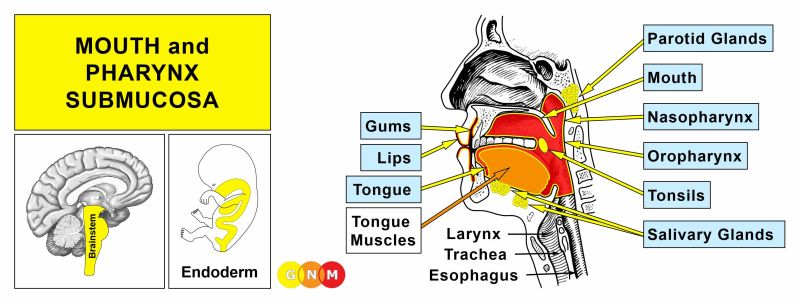 DEVELOPMENT AND FUNCTION OF THE MOUTH AND PHARYNX SUBMUCOSA: The mouth is the opening of the alimentary canal and the place where the digestion (secretory quality) and absorption (absorptive quality) of food starts. The tongue is an accessory digestive organ that aids in chewing and swallowing. Through chewing, food is broken into small pieces. Saliva produced in the salivary glands moistens the food bolus to make swallowing easier. The salivary glands are located in several parts of the mouth. The largest salivary glands are the parotid glands in front of the ears, the sublingual glands underneath the tongue, and the submandibular glands beneath the lower jaw. The pharynx connects the mouth and nasal cavities with the trachea and the larynx. The nasopharynx, located in the back of the nose, extends to the upper surface of the palate which forms the roof of the mouth; the oropharynx is at the very back of the mouth. On both sides of the pharynx lie the tonsils. Branching off the pharynx is the esophagus that carries food from the mouth to the stomach. The submucosa of the mouth and pharynx (including the lips, gums, palate, tongue, salivary glands, tonsils, and throat) consists of intestinal cylinder epithelium, originates from the endoderm and is therefore controlled from the brainstem.
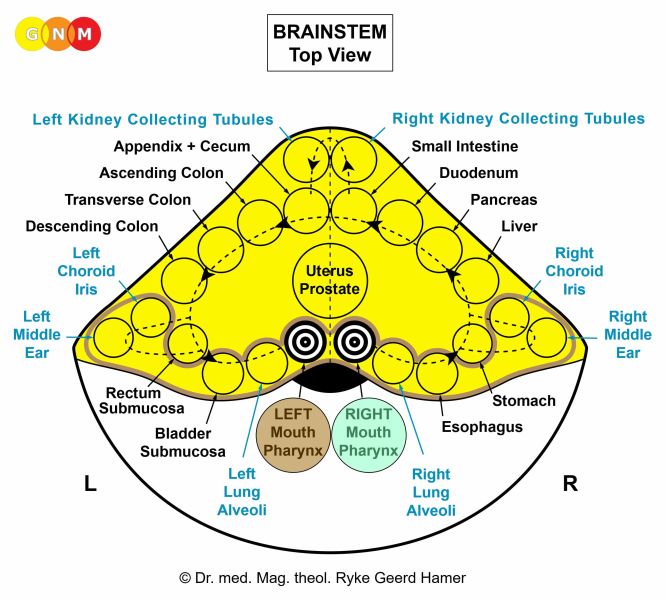 BRAIN LEVEL: In the brainstem, the organs of the mouth and pharynx have two control centers that are orderly positioned within the ring form of the brain relays that control the organs of the alimentary canal.
The right half of the mouth and pharynx is controlled from the right side of the brainstem; the left half is controlled from the left brainstem hemisphere. There is no cross-over correlation from the brain to the organ.
NOTE: The mouth and pharynx, tear glands, Eustachian tubes, thyroid gland, parathyroid glands, pituitary gland, pineal gland, and choroid plexuses share the same brain relays.
BIOLOGICAL CONFLICT: The biological conflict linked to the submucosa of the mouth and pharynx, including the lips, gums, palate, tongue, salivary glands, tonsils, and throat is a “morsel conflict” (compare with “morsel conflict” related to the stomach, duodenum, pancreas gland, small intestine, colon, and thyroid gland).
RIGHT HALF OF THE MOUTH AND PHARYNX
 Based on the original function of the gullet, the right half of the mouth and pharynx correlates to an “ingoing (food) morsel” and to “not being able to catch a morsel” (mouth, lips, gums, palate, tongue, salivary glands) or “not being able to swallow a morsel” (tonsils, pharynx, throat).
Newborns and infants experience the conflict in real terms when they can’t get the “milk morsel”, let’s say, because the mother is not able to nurse or is not feeding her baby in time. Seniors in nursing homes and hospital patients suffer the conflict when they are unable to eat because of pain; also cancer patients who are not able to eat as a result of chemo treatments. Having to refrain from eating one’s favorite food (e.g., being put on a strict diet) can also cause a morsel conflict.
A figurative morsel one is not able to “catch” refers to something that one had expected or was looking forward to “grab” and “swallow” and is unexpectedly not able or not allowed to (see also biological conflict linked to the lower third of the esophagus). Such a desired “morsel” could be a deal, a contract, a business, a job, a position, a promotion, a “money morsel” in form of a loan, a profit, a gift, or an inheritance (house, apartment); for children it could be a “toy morsel” or a “good grade morsel”. The conflict might also concern a person one cannot “catch” or “get a hold of” or a relationship one is not able or not allowed to “consume”.
The right half of the nasopharynx relates to a “scent morsel” one is unable to catch, for example, the scent of a loved one who has left.
LEFT HALF OF THE MOUTH AND PHARYNX
 Originally, before the rupture of the gullet, the biological conflict related to the outgoing section of the intestine was “not being able to sufficiently insalivate the fecal morsel”, because mucus produced in the gullet also served the lubrication of feces to facilitate elimination. Today, the conflict linked to the left half of the mouth and pharynx correlates to an “outgoing (food) morsel” and to “not being able to eliminate a morsel (spit it out)”.
This refers, for example, to food or medication one wants to “puke out”. An undesirable morsel might be associated with a commitment or promise one wants to revoke or an agreement one wants to call off. A newly hired employee, a new tenant or roommate, a new sibling, or an annoying visitor could be perceived as a “morsel” one wants to get rid of. In sports, it could relate to not being able to pass the ball (soccer) or puck (hockey). An “outgoing morsel” can also be a word or words one is not allowed or unable to “spit out”, for instance, an apology, a confession, a plea, or a complaint. Unwanted or forced oral sex might evoke the conflict.
The left half of the nasopharynx relates to a “scent morsel” one is unable to get rid of, for example, the scent of an opponent or of a competitor.
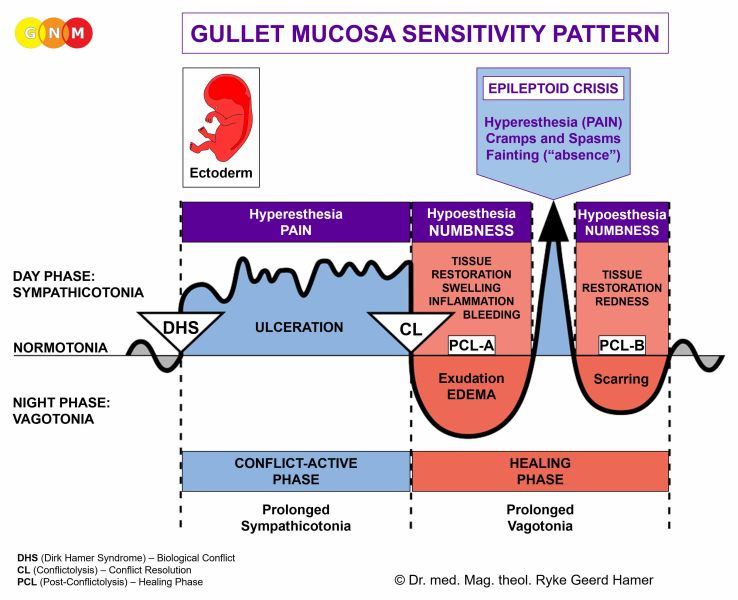
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the submucosa of the mouth or pharynx proliferate proportionally to the intensity of the conflict. The biological purpose of the additional cells is to better insalivate a morsel in order to absorb (right half) or expel (left half) it faster. Salivation is stimulated by the autonomic nervous system. This is why the secretion of saliva increases with the smell of “mouth-watering” food. In the English language, “salivating” and “drooling” are synonyms for “craving” for something or someone desirable.
With prolonged conflict activity a flat growth (absorptive type) develops in the submucosa of the mouth. In the palate, salivary glands, tonsils, pharynx, and throat it can also take a cauliflower-shaped form (secretory type). If the papillae of the tongue that contain the taste buds are affected, the additional cells provide an enhanced sense of taste in order to be able to analyze (see sensory quality) the “morsel” (compare with hypersensitivity to taste related to the posterior third of the tongue).
A large growth is usually diagnosed as an oral cancer (compare with “oral cancer” related to the mouth surface mucosa) or as a “glandular tumor” if it involves the salivary glands.
Smoking and alcohol abuse are said to be risk factors for cancers in the mouth, including tongue cancer. Yet, not everybody who smokes or drinks develops oral cancer. If, however, the “cigarette morsel” or the “alcohol morsel” causes distress, for example, due to abstinence, withdrawal, or a fear of getting mouth or tongue cancer, the Biological Special Program will be set into motion.
 On a CT scan, the conflict-active phase of a “morsel conflict” presents as a Hamer Focus with a sharp ring configuration. Here, on the right brainstem hemisphere in the brain relay of the submucosa of the right side of the mouth (view the GNM diagram). At this point, the conflict of “not being able to catch a morsel” is still active.
Adenoids in the nasopharynx form as a result of a hanging conflict, that is, when the “scent morsel”-conflict cannot be resolved in time (compare with polyps in the paranasal sinuses). If the tonsils are affected, this causes tonsillar hypertrophy, or enlarged tonsils. Since the tonsils and the nasopharynx share the same brain relay, nasal polyps and enlarged tonsils often occur together.
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed.
In the mouth, the healing phase presents as canker sores (aphthous ulcers) on the inside of the lips or cheeks, on the palate or tongue, or in all areas of the mouth, depending on the perception of the conflict situation (compare with aphthous ulcers related to the mouth surface mucosa). Canker sores appear as round or oval white spots with an inflamed border. They can be quite painful. On the gums, the pus-filled pocket is called a “dental abscess” or gum abscess. The tuberculous discharge causes bad breath.
 A canker sore on the right side of the mouth (here on the inside of the lower lip) indicates that the conflict of “not being able to catch a morsel” is resolved and that healing is underway.
If the required microbes are not available upon the resolution of the conflict, the additional cells remain. Eventually, the growth becomes encapsulated with connective tissue. In conventional medicine, this is usually diagnosed as a mouth polyp or “benign cancer”. A gum polyp might reach into the neck of a tooth.
 Oral candidiasis or thrush, presenting as creamy pus, occurs when fungi assist the healing process. Babies typically develop thrush when they suffer the distress of not getting the “milk morsel”.
 Tonsillitis, an inflammation of the tonsils, is a sign that the related morsel conflict has been resolved (the picture shows an inflammation of the left tonsil, corresponding to “not being able to eliminate a morsel”). When pus, produced during the healing process (purulent tonsillitis), is released into the mouth, this causes a smelly breath. Here we also find tonsil abscesses.
Tonsillar mycosis or candidiasis of the tonsils indicates the presence of fungi (compare with “strep throat” with the involvement of streptococcus bacteria).
In the nasopharynx, adenoids or nasal polyps that developed during the conflict-active phase are removed with the help of fungi or TB bacteria, provided they are available. The nasal discharge consists of smelly tubercular secretion. A nasal abscess with painful swelling containing pus also develops in the healing phase.
 What is termed Zenker's diverticulum is a pouch at the lower level of the pharynx (just above the upper esophageal sphincter) that develops as a result of a hanging healing. Because of the continuous bacterial cell removal process, the wall of the pharynx becomes thin and the weakest portion of the pharyngeal wall balloons out, forming a diverticulum (compare with diverticula in the colon). The most common symptom of Zenker's diverticulum is difficulty swallowing food.
In the salivary glands, a prolonged healing process (hanging healing) leads to a complete loss of the saliva-producing acinar cells resulting in a permanently dry mouth or what is called Sjogren’s or Sicca syndrome (see also dry mouth related to the salivary gland ducts and Sjogren’s associated with dry eyes). An inflammation in the salivary glands, for example, in the parotid glands causes parotitis, also known as mumps (see also parotitis related to the salivary gland ducts).
|
 DEVELOPMENT AND FUNCTION OF THE MOUTH AND PHARYNX SURFACE MUCOSA: The submucosa of the mouth and pharynx is covered with a cell layer composed of squamous epithelium, which derives from the ectoderm and is therefore controlled from the cerebral cortex. NOTE: The tonsils do not have an ectodermal surface mucosa.
 BRAIN LEVEL: The epithelial lining of the mouth and pharynx, including the surface mucosa of the throat, is controlled from the pre-motor sensory cortex (part of the cerebral cortex). The right half of the mouth and pharynx is controlled from the left side of the cortex; the left half is controlled from the right cortical hemisphere (medio-fronto-basal). Hence, there is a cross-over correlation from the brain to the organ. The brain relays of the tongue and throat are located laterally.
MOUTH SURFACE MUCOSA
BIOLOGICAL CONFLICT OF THE MOUTH SURFACE MUCOSA: The biological conflict linked to the mouth surface mucosa (including the lips, gums, palate, and tongue) is an oral conflict of either “not being able to take something into the mouth” or, the opposite, of “not being able to get rid of something that is in the mouth or on the tongue”. In both cases, this concerns food one desires but is unable or not allowed to “take in” (being on a restricted diet, e.g., diabetics) or food one wants to “spit out”. Regarding the latter, this differs distinctively from the conflict of “not being able to eliminate a morsel” linked to the left half of the mouth submucosa. While the deep endodermal layer of the mouth correlates biologically to the actual morsel (real or figurative) one wants to expel, the upper ectodermal layer is rather about contact with the “morsel”, namely, wanting to separate from what is in the mouth (see separation conflict related to the epidermis). Conversely, the conflict of not being able to get something desirable into the mouth can be triggered by having to refrain from cigarette smoking or alcohol. A lip-related conflict translates into the loss of physical contact or the fear of losing contact associated with the lips, for example, if one is no longer able or allowed to kiss a person or a pet. Equally, it also applies to not wanting to be kissed or having tongue or lip contact. This includes contact with objects such as a drinking glass, a straw, eating utensils, dental tools, and the like. In a figurative sense, the oral conflict translates into not being allowed or able to say something that is “on the tip of the tongue”.
CONFLICT-ACTIVE PHASE: ulceration in the epithelial mouth mucosa proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the oral cavity in order to facilitate the intake of or the separation from the “morsel”. With an intense conflict aphthous ulcers develop at the site (compare with canker sores related to the mouth submucosa). If the oral conflict is associated with the tongue, this causes tongue burning.
 This brain CT shows conflict activity of an oral conflict with aphthous ulcers on both sides of the mouth. The Hamer Focus reaches over both brain hemispheres. In GNM, we call this a “central conflict”, meaning that the conflict was associated with the person’s mother/child and partner at the same time. An adolescent caught smoking by his/her parents would be a classic conflict scenario.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation. Healing symptoms are swelling, water-filled blisters, redness (see “raspberry tongue” with scarlet fever), and possibly bleeding. On the lips, such blisters are commonly called “cold sores” or “herpes” (see also herpes related to the epidermis).
  For a right-handed person, a blister on the left half of the tongue reveals a mother/child-related oral conflict (the story: a right-handed teenage girl was caught tongue-kissing by her mother).
The CT scan presents the Hamer Focus in the area of the brain from where the left half of the tongue is controlled (view the GNM diagram).
Gingivitis is restricted to the gum tissue. An inflammation of the gums might also arise during the healing of periodontosis. In this case, the condition is called periodontitis. In today’s dentistry, it is wrongly assumed that “gum diseases” are caused by dental plaque.
 Here we see gingivitis exclusively on the left side of the mouth (see red arrows). For a left-handed person this indicates that the conflict was associated with a partner.
The inflamed area of the gums might bleed during teeth brushing and flossing (compare with gum bleeding related to the dentin SBS).
 A gum abscess originates in the mouth submucosa. Here we see a gum abscess on the right side of the mouth related to “not being able to catch a morsel”. The pus-filled abscess develops in the healing phase.
An intense healing phase with a large swelling in the mouth area might be diagnosed as an “oral cancer” (compare with oral cancer related to the mouth submucosa). Based on the knowledge of GNM, the new cells cannot be regarded as “cancer cells” since the cell increase is, in reality, a replenishing process.
 This picture shows acute swelling on the right side of the hard palate. It is a positive sign that the related oral conflict has been resolved. Water retention due to the SYNDROME increases the swelling significantly.
PALATE AND TONGUE
BIOLOGICAL CONFLICT OF THE BACK OF THE PALATE AND POSTERIOR THIRD OF THE TONGUE: The biological conflict linked to the soft palate is “wanting to get rid of something that is on the palate” (dental tools). The back of the tongue relates to “not being able or not wanting to taste something” (certain foods or liquids).
CONFLICT-ACTIVE PHASE: ulceration in the epithelial lining of the palate and/or tongue (posterior parts) proportional to the degree and duration of conflict activity. Symptoms: painful ulcers in the back of the palate or tongue with a hypersensitivity to taste (in Nature, the sensory perception of a spoiled “food morsel” or poison is essential for survival).
HEALING PHASE: The ulceration in the palate and/or tongue is refilled and replenished. The affected area is swollen and might bleed. During PCL-A and PCL-B there is a hyposensitivity to taste (compare with a loss of sense of taste with facial paralysis).
PHARYNX AND THROAT
BIOLOGICAL CONFLICT OF THE PHARYNX AND THROAT SURFACE MUCOSA: Like the conflict linked to the upper two-thirds of the esophagus to which the pharynx and throat connect, the biological conflict corresponding to the pharynx and throat surface mucosa is “not wanting to swallow a morsel”. Figuratively, this refers to any incident or situation one refuses to accept or which is perceived as hard to “swallow”.
CONFLICT-ACTIVE PHASE: ulceration in the epithelial lining of the pharynx and throat proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the lumen of the pharynx and throat in order to be better able to eliminate the undesirable “morsel”. The ulceration causes a sore throat, explicitly, a scratchy throat.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation. Healing symptoms are swelling due to the edema (fluid accumulation), difficulties swallowing (a thick and tight throat) with pain (in PCL-A and PCL-B the pain is not of a sensory nature but rather pressure pain). Concurrent water retention due to the SYNDROME enlarges the swelling and therefore increases the pain. With an inflammation, the condition is called pharyngitis, typically accompanied by fever.
What is commonly called a strep throat indicates that the healing process is assisted by streptococcus bacteria. This is generally the case when the ulceration that takes place in the conflict-active phase reaches deep into the epithelial tissue.
|
 DEVELOPMENT AND FUNCTION OF THE SALIVARY GLAND DUCTS: Saliva, produced in the salivary glands (sublingual glands, submandibular glands, parotid glands) reaches the oral cavity through the salivary gland ducts. The moisturizing function of saliva allows to insalivate the “food morsel” so that it can pass easily from the mouth into the esophagus. The lining of the salivary gland ducts consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
 BRAIN LEVEL: The epithelial lining of the salivary gland ducts is controlled from the pre-motor sensory cortex (part of the cerebral cortex). The right salivary gland ducts are controlled from the left side of the cortex; the left salivary gland ducts are controlled from the right cortical hemisphere (fronto-lateral-basal). Hence, there is a cross-over correlation from the brain to the organ.
BIOLOGICAL CONFLICT: Based on the role of saliva in the insalivation of food, the biological conflict linked to the salivary gland ducts is “not being able to eat” or “not being allowed to eat”. Children experience the conflict when they don’t get a desired “food morsel” (chocolate, ice cream, candy), but also adults, particularly women, when they don’t allow themselves to eat in order to lose weight. People on strict diets, including diabetics, are more susceptible to suffer the conflict.
CONFLICT-ACTIVE PHASE: ulceration in the salivary gland duct(s) proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the ducts so that more saliva can be delivered to the mouth to facilitate the insalivation of food. Symptom: pain ranging from mild to severe.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation with swelling due to the edema (fluid accumulation) in the healing area. With concurrent water retention (the SYNDROME) the increased swelling might obstruct the salivary gland ducts causing parotitis, or mumps. Mumps is not only a “children’s disease” but also affects adolescents and adults. The theory that men who “contract mumps” after puberty have the risk of developing orchitis, an inflammation of the testicles, has no scientific basis. Besides, the existence of a “mumps virus” has never been substantiated.
MUMPS develops in the healing phase of “not being able or not being allowed or being unwilling to eat” with swelling in the parotid gland ducts or of “not being able to catch a morsel” (right side) or “not being able to eliminate a morsel” (left side) involving the parotid gland.
 This picture shows hockey star Sidney Crosby of the Pittsburgh Penguins with mumps (parotitis) on his right side. The distress of not being able to catch the “puck morsel” (e.g., not being in the lineup for playing a game) is a possible conflict scenario.
Prolonged healing because of continuous conflict relapses results in a permanent blockage of the saliva flow causing a dry mouth. This condition is called Sjogren’s or Sicca syndrome (see also dry mouth related to the mouth submucosa and Sjogren’s related to dry eyes). Conventional medicine argues that Sjogren’s is linked to a low estrogen level since it affects predominantly women after menopause. However, not every postmenopausal woman has Sjogren’s! From the GNM perspective, the increasing rate of the “dry mouth syndrome” is not at all related to a woman’s hormone level but rather to today’s diet-mania and more women experiencing the distress of “not being allowed to eat”. The theory that Sjogren’s is an autoimmune disease, suggesting that the body’s immune system “mistakenly” attacks its own body cells, is in light of the Five Biological Laws pointless.
A salivary gland duct stone is a calcified structure that forms inside a salivary gland duct (in the sublingual gland or submandibular gland) as a result of a hanging healing. A large stone can also block the flow of saliva into the mouth.
|
 DEVELOPMENT AND FUNCTION OF THE TONGUE MUSCLES: The tongue is a muscular organ covered by an endodermal submucosa and an ectodermal surface mucosa. The tongue coats food with saliva, aids in chewing and pushing food into the pharynx from where it goes through the esophagus into the gastrointestinal tract. Next to chewing and swallowing, the tongue assists in speech and the formation of words. The tongue consists of striated muscles, originates from the new mesoderm and is therefore controlled from the cerebral medulla and the motor cortex.
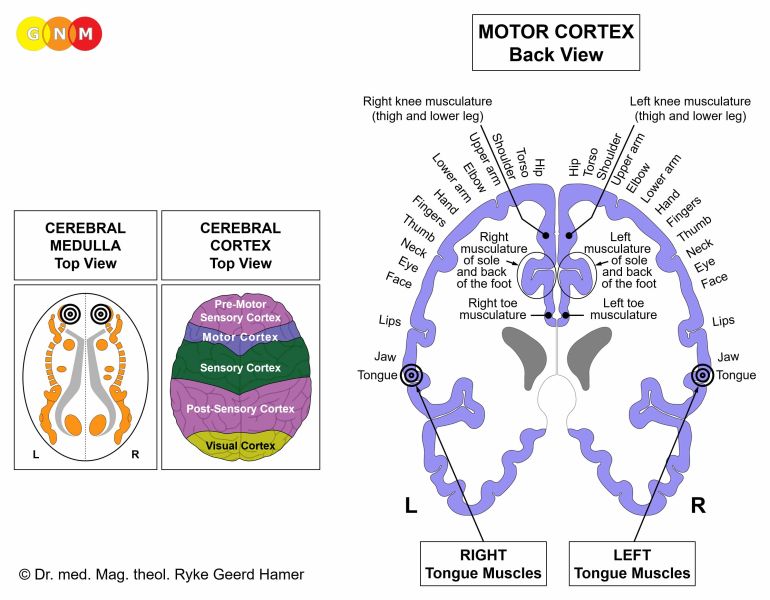 BRAIN LEVEL: The tongue has two control centers in the cerebrum. The trophic function of the tongue muscles, responsible for the nutrition of the tissue, is controlled from the cerebral medulla; the ability to move the tongue is controlled from the motor cortex (part of the cerebral cortex). The right half of the tongue is controlled from the left side of the cerebrum; the left half is controlled from the right cerebral hemisphere. Hence, there is a cross-over correlation from the brain to the organ (see GNM diagram showing the motor homunculus).
BIOLOGICAL CONFLICT: The biological conflict linked to the tongue muscles is “not being able to pull the tongue away” (contact with hot liquids or hot food) or “not being able to move the tongue”. A difficult dental procedure or intubation could cause such tongue-related distress; also, sexual abuse (oral sex, forced tongue kissing). Considering the function of the tongue in articulation and talking, not being able to speak or not being allowed to speak (to get a word off the tongue) can also trigger the conflict. The masticatory muscle relates to the conflict of “not being able to chew” (e.g., with braces or dentures).
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of tongue muscle tissue (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing paralysis of the tongue muscles (controlled from the motor cortex) affecting speech and swallowing (see also stroke and tongue paralysis). Whether the right or left side of the tongue is affected is determined by a person’s handedness and whether the conflict is mother/child or partner-related.
HEALING PHASE: During the healing phase the tongue muscle tissue is reconstructed. The paralysis reaches into PCL-A. After the Epileptoid Crisis, during PCL-B, the function of the tongue returns to normal.
 This brain CT presents a Hamer Focus in the scarification phase (PCL-B). The accumulation of neuroglia (visible as white) in the area of the motor cortex controlling the muscle of the right half of the tongue (view the GNM diagram) indicates that the tongue-related conflict has been resolved. In conventional medicine, the glia buildup is wrongly assumed to be a “brain tumor”.
| ||||||||||||||||