Male Sexual Organs

DEVELOPMENT AND FUNCTION OF THE PROSTATE GLAND: The prostate is located in the male pelvis just below the bladder. The urethra, which carries both urine and semen, passes through the center of the prostate from where it extends to the head of the penis. The main function of the prostate gland is to secrete seminal fluid (secretory quality). During sexual arousal, a considerable portion of semen is also produced in the seminal vesicle, a sac-like pouch that opens into the ejaculatory duct that joins with the prostatic urethra. Seminal fluid provides sperm cells with energy and aids in their motility. One of the components of prostatic secretion is the so-called PSA-Prostate Specific Antigen (see also “female prostate” or Skene’s gland). Prostatic fluid contains the fragrance that gives semen its typical musky scent. In Nature, the odor of the seminal scent-mark signals the female sexual potency and male strength. The prostate gland consists of intestinal cylinder epithelium, originates from the endoderm and is therefore controlled from the brainstem.

BRAIN LEVEL: The prostate gland is controlled from the center of the brainstem.
BIOLOGICAL CONFLICT: Consistent with its vital role in reproduction, the biological conflict linked to the prostate gland concerns procreation (equal to the uterus in females). A man can suffer a procreation conflict when he is unable to father children, for instance, due to erectile dysfunction or infertility, including his partner’s inability to conceive (female infertility). A vasectomy (surgical sterilization) might evoke a procreation conflict on a subtle psycho-biological level. Males also experience the conflict when their descendants don’t reproduce, let’s say, because of a homosexual orientation, staying childless by choice, miscarriages, or abortions. The male prostate also correlates to a mating conflict or sexual conflict. In the human world, “not being able to mate” or “not being allowed to mate” translates into sexual rejection and feeling sexually unwanted (compare with female mating conflict related to the cervix uteri). Mating conflicts are activated through the loss of a sexual mate or through sexual rivalry (the “fight over a female”). A man’s fear that his sexual mate is attracted to another man could already trigger the conflict, especially when the competitor is younger or has more “potential”. In addition, the prostate corresponds to a gender conflict experienced as an “ugly conflict with a female”. Being dominated, controlled, or humiliated by a woman (an imperious wife or mother) or degraded by a female authority (supervisor, judge, lawyer, doctor, police officer, and the like) can go straight to a man’s prostate. A spiteful divorce, custody battles, emotional or financial abuse are other possible conflict scenarios. In a broader sense, the prostate-related conflict concerns maleness itself, in the sense of being disregarded as a man, as a lover, as a husband, or as the provider of the family.
NOTE: A male with a normal hormone status, that is, when his testosterone level is higher than his estrogen level, experiences a sexual conflict as a male sexual conflict affecting the prostate. With a low testosterone status he perceives the conflict as a female sexual conflict linked to the coronary veins, controlled from the left temporal lobe of the cerebral cortex (see Principle of Gender, Laterality, and Hormone Status).
A male with a low testosterone status is no longer able to experience a territorial conflict (territorial fear conflict, territorial loss conflict, territorial anger conflict, territorial marking conflict) in biological terms. Dr. Hamer established that a (territorial) fear, (territorial) anger, (territorial) loss, or (territorial) marking conflict involving a female affects, therefore, also the prostate.
|
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase prostate gland cells proliferate proportionally to the intensity of the conflict. The biological purpose of the additional cells is to increase the amount of semen in order to enhance the chance of impregnating a female once a sexual mate becomes available. With prolonged conflict activity (hanging conflict) a growth (secretory type), referred to as a prostate cancer, develops as a result of the continuing cell augmentation (compare with “prostate cancer” related to the prostatic ducts). If the rate of cell division exceeds a certain limit, conventional medicine considers the cancer as “malignant”.
Hormone therapies, the standard treatment for prostate cancer, are aimed at “slowing the growth of the cancer” by suppressing the production of male hormones such as testosterone (based on the assumption that androgens stimulate prostate cancer cells to grow). Side effects of the drugs are erection problems, breast tenderness, and hot flashes. The reason why the “therapy” seems to work is that the hormonal manipulation changes a man’s biological identity. As a result, the originally male conflict (procreation conflict, mating conflict, gender conflict) becomes irrelevant and the prostate tumor shrinks.
During conflict activity the PSA level rises at the same rate as the cell proliferation in the prostate gland.
NOTE: Strictly speaking, the term “PSA-Prostate Specific Antigen” is a misnomer because so-called PSA is also produced in the liver, lungs, or salivary glands. This explains why men whose prostate has been removed might still show an elevated PSA level. Even female organs such as the breast and the Skene's gland produce “PSA” (Source: The New England Journal of Medicine, September 21, 2000).
|
Conventional medicine uses PSA as a tumor marker, whereby a serum PSA level higher than 4 ng/ml is regarded as “abnormal”. Based on this consensus, prostate cancer became quickly the leading cancer in men, just as breast cancer became the most common cancer in women with the introduction of mammography.
Questioning PSA Screening
Founded on latest research, the American Society of Clinical Oncology and the American College of Physicians concluded that “it is uncertain whether the benefits associated with PSA testing for prostate cancer screening are worth the harms associated with screening and subsequent unnecessary treatment” (Journal of Clinical Oncology, August 2012).
|
Oftentimes, a positive PSA test and a subsequent prostate cancer diagnosis lead to radiation treatments or surgery. After a radical prostatectomy (removal of the prostate) most men are left with urinary incontinence and erectile dysfunction, which in turn causes self-devaluation conflicts affecting the bones closest to the prostate. Bone cancer of the pubic bone or lower spine is therefore next to lung cancer (death-fright conflict) the most frequent secondary cancer in men. It has nothing to do with “migrating cancer cells” (“metastasis”).
If the prostate tumor is found in the lateral lobes of the prostate, it is usually diagnosed as a “cancer”. What is termed benign prostate hyperplasia (BHP) is an augmentation of prostate gland cells in the central portion of the prostate causing a general enlargement of the prostate gland (the same diagnostic standard is applied to endometrial hyperplasia related to the uterus). Typically the cell proliferation occurs on a flat plane (compare with prostate hyperplasia related to the prostatic ducts). If the swelling presses on the urethra, the urine flow is delayed and slow with only small amounts of urine being expelled (see also healing phase). According to Dr. Hamer, a prostate enlargement occurs when a prostate-related conflict becomes more of an overall “issue”, for example, if a man feels that he is no longer attracting females as he used to. Also, when a man gets older, his testosterone level decreases; so does his sex drive. This is a normal part of the aging process. However, the pressure to “perform” (also self-inflicted pressure) can easily cause a mating conflict. These are all factors that explain why “benign prostate hyperplasia” is attributed primarily to older men and why PSA levels tend to increase with age. However, the changes are always linked to a biological conflict. This is why not all men have elevated PSA levels when they get older.
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. The discharge produced during the cell (tumor) breakdown is excreted through the urethra. Thus, the urine is cloudy, potentially mixed with blood (as to blood in the urine, see also healing phase related to the bladder trigone, bladder mucosa, and kidney parenchyma). Blood might be in the ejaculate as well. The healing process is accompanied by night sweats. With an inflammation, the condition is called prostatitis. Candidiasis involving the male genital organs originates in the prostate gland, the smegma producing glands, or in the corium skin covering the penis and the scrotum.
With a hanging healing, that is, when healing is continually interrupted by conflict relapses, the prolonged decomposing process results in a loss of prostate gland tissue. The lack of seminal fluid production is the underlying cause of a dry orgasm, an orgasm without ejaculating any semen (compare with dry orgasm related to the ejaculatory ducts). The same happens after a surgical removal of the prostate.
If the swelling is in a location that it presses onto the prostatic urethra, this causes a delayed and slow urination (see also conflict-active phase). A large swelling might compress the urethra completely with urine flowing back into the kidneys. Should an obstruction of the urethra arise, Dr. Hamer recommends the use of a catheter until the healing process has been completed and the normal urine flow restored (see also urinary tract obstruction related to the urethra).

This brain CT belongs to a man who is in the healing phase of a prostate cancer. The fluid accumulation (PCL-A) in the prostate gland relay (view the GNM diagram) occurs parallel to the swelling (edema) on the healing organ.
After the completion of the healing phase, the prostate gland regains its normal size and the PSA level returns to normal. However, with recurring conflict relapses the PSA level fluctuates up and down in synchronicity with the degree of the reactivated conflict.
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells remain. The tumor that cannot be broken down eventually encapsulates. As a result, the delayed urination becomes permanent. The PSA level continues to be elevated! If the tumor blocks the urethra, surgery is inevitable.

DEVELOPMENT AND FUNCTION OF THE PROSTATIC AND EJACULATORY DUCTS: The prostatic ducts lie within the prostate. They carry the fluid secreted by the prostate gland into the prostatic portion of the urethra, where the secretion blends with the seminal fluid from the seminal vesicles. The two ejaculatory ducts that deliver sperm from the testicles and fluids from the seminal vesicles also open into the urethra. During ejaculation, semen is expelled through the urethral opening at the tip of the penis. The walls of the prostatic and ejaculatory ducts are endowed with smooth muscles. Equal to the intestinal muscles that move the “food morsel” along the intestinal canal through peristaltic motion, the smooth muscles of the prostatic and ejaculatory ducts facilitate the flow and elimination of the “semen morsel”. The lining of the prostatic and ejaculatory ducts consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.

BRAIN LEVEL: The epithelial lining of the prostatic and ejaculatory ducts is controlled from the temporal lobes (part of the post-sensory cortex). The prostatic ducts in the right half of the prostate and the right ejaculatory duct are controlled from the left side of the cortex; the prostatic ducts in the left half of the prostate and the left ejaculatory duct are controlled from the right cortical hemisphere. Hence, there is a cross-over correlation from the brain to the organ.
NOTE: The prostatic ducts, ejaculatory ducts, renal pelvis, ureters, bladder, and urethra share the same brain relays and therefore the same biological conflict.
BIOLOGICAL CONFLICT: The biological conflict linked to the prostatic ducts and ejaculatory ducts is the same as for the urethra, namely a territorial marking conflict. In this case, the marking conflict has a sexual nuance or a distinctive “prostate quality”. A man can suffer the conflict when, for example, his ex-wife doesn’t allow him to see his children or when his space is invaded by a sexual rival or by a domineering female. The ejaculatory ducts also relate to an ejaculation conflict (see also urethra) as in “not being able, not being allowed, or not wanting to ejaculate” (for example, premature ejaculation).
In line with evolutionary reasoning, territorial conflicts, sexual conflicts, and separation conflicts are the primary conflict themes associated with organs of ectodermal origin, controlled from the sensory, pre-motor sensory and post-sensory cortex.
|
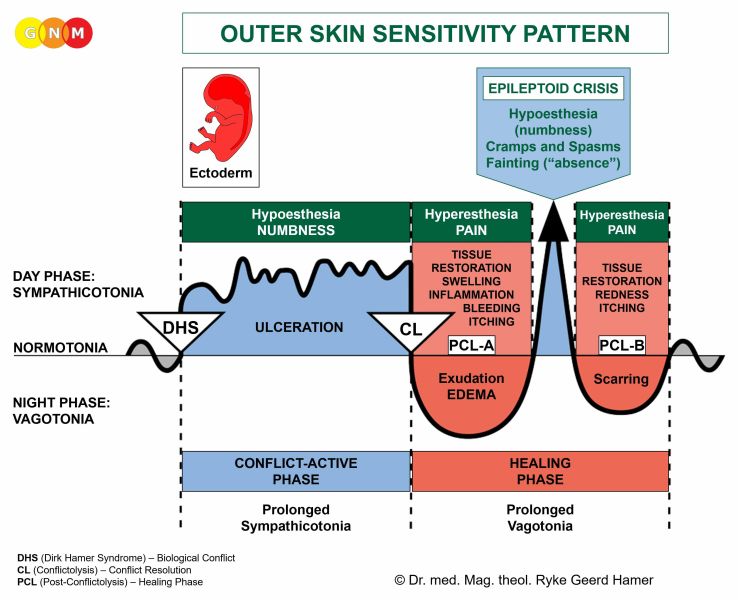 The Biological Special Program of the mucosa of the prostatic ducts follows the OUTER SKIN SENSITIVITY PATTERN with hyposensitivity during the conflict-active phase and the Epileptoid Crisis and hypersensitivity in the healing phase.
|
CONFLICT-ACTIVE PHASE: ulceration (cell loss) in the lining of the prostatic ducts or ejaculatory ducts proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the ducts to improve the flow of semen to be better able to mark the (sexual) territory.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss in the prostatic ducts is replenished through cell proliferation with swelling due to the edema (fluid accumulation). Water retention brought on by an active abandonment or existence conflict (the SYNDROME) increases the swelling causing an enlarged prostate. Conflict relapses delay the completion of the healing process. NOTE: Contrary to a prostate enlargement related to the prostate gland, the PSA level stays within the normal range.
If the preceding conflict-active phase was intense and lasted over a long period of time, the profuse cell proliferation that occurs during PCL-A is diagnosed as an intraductal prostate cancer (compare with prostate cancer related to the prostate gland). Based on the Five Biological Laws, the new cells cannot be regarded as “cancer cells” since the cell increase is, in reality, a replenishing process.
Gonorrhea (see urethral gonorrhea) can also originate in the prostatic ducts. If the symptoms (inflammation, discharge) are less severe, the condition is usually diagnosed as prostatitis.
An ejaculatory duct obstruction occurs due to the swelling in one or both ejaculatory ducts during the healing phase. Conflict-related tracks or conflict relapses prolong the healing process. Ejaculatory duct obstruction is an underlying cause of a dry orgasm (compare with dry orgasm related to the prostate gland) and of male infertility (see also male infertility related to the testicles).
PROSTATE GLAND
|

DEVELOPMENT AND FUNCTION OF THE MALE GERM CELLS: In the human reproductive organs, germ cells are the cellular units that give rise to gametes (sperms and eggs). The primordial germ cells appear first in the yolk sac of the embryo from where they migrate through the developing intestine to the new gonads (testicles or ovaries). In the testicles, the germ cells form so-called spermatogonia (secretory quality), which are precursor cells of sperms. Beginning with puberty, spermatogonia start to develop into mature sperm cells. This process, called spermatogenesis, takes place in the seminiferous (sperm-producing) tubules of each testicle and continues to old age (oogenesis, the creation of egg cells in the female ovaries, lasts only until menopause). Germ cells derive from the endoderm and are controlled from the midbrain.

BRAIN LEVEL: The male (and female) germ cells are controlled from the midbrain, located at the outermost part of the brainstem. The germ cells in the right testicle are controlled from the right side of the midbrain; the germ cells in the left testicle from the left side (compare with interstitial cells of the testicles).
BIOLOGICAL CONFLICT: The biological conflict linked to the germ cells is a profound loss conflict, often the loss of a child (compare with loss conflict related to the testicles).
CONFLICT-ACTIVE PHASE: During the conflict-active phase a testicular teratoma (secretory type), or germ cell tumor, develops in the testicles (see also ovarian teratoma in females). The significance of a teratoma relates to the primeval ability of parthenogenesis, the reproduction without fertilization. The biological purpose of the additional germ cells is to facilitate faster reproduction in the emergency of the loss of an offspring. In conventional medicine, a “malignant teratoma” is classified as a testicular cancer (compare with “testicular cancer” related to the testicles); a “malignant germ cell tumor” is also referred to as a seminoma.
NOTE: The cell proliferation that takes place with the growth of a teratoma is the same as it occurs in the development of the fetus. During the first three months of pregnancy, the cell increase follows the principle of old brain-controlled organs with cell proliferation in sympathicotonia (conflict-active phase). Starting at the fourth month of gestation, the cell proliferation follows the pattern of cerebrum-controlled organs with cell proliferation in vagotonia (healing phase).
|
HEALING PHASE: With the conflict resolution (CL), the teratoma stops growing only slowly since embryonic tissue develops in spurts (“fetal growth spurt”). During the healing phase, fungi or mycobacteria such as TB bacteria may decompose the teratoma, provided they are available. The swelling filled with pus presents as a testicular abscess. The healing process is accompanied by night sweats. If the teratoma remains, the growth encapsulates. Remarkably, an encapsulated teratoma, termed a dermoid cyst, might contain structures such as hair, teeth, or bones. Teratoma or dermoids are also found in the spinal area, that is, in close vicinity to where the testicles originate during the fetal development.
 “The discovery of the New Medicine began with the death of my son Dirk. On August 18, 1978, Dirk was shot near the Mediterrean island of Cavallo/Corsica by the Italian Crown Prince Vittorio Emanuele of Savoy. Three and a half months later, on December 7, 1978, Dirk succumbed to his injuries and died in my arms at the University Clinic in Heidelberg…
|
 … now I am aware that on that day, I had suffered a profound loss conflict with the development of a testicular cancer. The biopsy revealed a testicular teratoma. At the time I underwent surgery. Today, with the understanding of the Iron Rule of Cancer, I would certainly never do so…” (Ryke Geerd Hamer).
|

DEVELOPMENT AND FUNCTION OF THE TESTICLES: In the male fetus, the development of the testicles starts in the abdominal cavity at the height of the upper lumbar region, approximately in the same area as the female ovaries. Around the seventh month of gestation, the testes descend into the scrotum. Like the peritoneum that covers the abdominal organs, a peritoneal layer (tunica vaginalis testis) envelops the testicles for protection. The testicles contain germ cells and interstitial cells (Leydig cells) that are responsible for the production of testosterone as well as small quantities of estrogen. Testosterone is required to transform germ cells into mature sperms with a head and a tail. The tail allows the sperms to propel into the epididymis at the surface of the testicle, where they are stored up to one month. When a male is sexually aroused, sperms enter the seminal duct. Mixed with the seminal fluids from the prostate gland and the seminal vesicles, semen empties into the urethra and is expelled during ejaculation. The testicles originate from the new mesoderm and are therefore controlled from the cerebral medulla.

BRAIN LEVEL: The testicles are controlled from the cerebral medulla, at the area where it adjoins the midbrain. The right testicle is controlled from the left side of the brain; the left testicle is controlled from the right cerebral hemisphere. Hence, there is a cross-over correlation from the brain to the organ.
BIOLOGICAL CONFLICT: The biological conflict linked to the testicles is a loss conflict concerning the loss of a loved one (see also loss conflict related to the ovaries). In comparison, the loss conflict related to the male germ cells is more of a primeval nature. The fear of losing a beloved person can already trigger the conflict. The same holds true for the loss of a pet. Constant self-blame after a break-up or death of someone close can keep the conflict active. A loss conflict can also be evoked through an argument, betrayal, or unfaithfulness of a partner or friend. NOTE: The loss conflict related to the testicles only concerns a person or a pet and NOT the loss of a home or of a business (see territorial loss conflict).
CONFLICT-ACTIVE PHASE: necrosis (cell loss) in the testicles, noticeable as light pulling in the scrotum. Because of the reduction of testosterone-producing cells the testosterone level decreases resulting in a reduced sperm production (see also low testosterone due to a conflict-related hormonal imbalance). Lasting conflict activity can, therefore, cause infertility, at least until the conflict is resolved.
NOTE: Whether the right or left testicle is affected is determined by a man’s handedness and whether the conflict is mother/child or partner-related.
|
HEALING PHASE: Starting with the conflict resolution (CL), the tissue loss is replenished with new cells. Healing symptoms are pain and swelling in the testicle. An inflammation or “infection” of a testicle (a sign that bacteria assist healing) is called orchitis. Conventional medicine claims that adult men who had “contracted mumps” in their teenage years are at risk of developing an inflammation of the testicles and will become infertile as a result of it. Yet, the theory does not explain why the alleged “mumps virus” would “attack” just the testicles; why the right testis or the left or both? However, the distress of not being able to father children, based on the “mumps causes infertility” myth, can certainly trigger a loss conflict.
A special characteristic regarding the healing of the testicles is the development of a TESTICULAR CYST. Provided there are no conflict relapses that interrupt healing, the process takes nine months to complete (see also ovarian cyst, kidney cyst, and adrenal cyst). The cyst formation occurs in several steps.
During PCL-A a fluid-filled capsule or cyst forms at the site of the necrosis. In order to restore the cell loss that occurred during the conflict-active phase, testicular cells proliferate inside the cyst. At this early stage, the cyst attaches itself to neighboring tissue for blood supply. Found during this period, the “growth” is usually diagnosed as a testicular cancer or Leydig cell tumor (compare with testicular cancer related to the germ cells). Based on the Five Biological Laws, the new cells cannot be regarded as “cancer cells” since the cell increase is, in reality, a replenishing process.

This brain CT shows an indistinct, partly edematous Hamer Focus in the area of the brain that controls the right testicle (view the GNM diagram), corresponding to a testicular cyst on the organ level. For a right-handed male, the loss conflict relates to a partner; for a left-hander to his mother or child.
After the Epileptoid Crisis, the cyst has lost most of its fluid. In PCL-B the cyst becomes hard, releases itself from the neighboring tissue and, endowed with blood vessels, integrates itself completely into the hormone-producing function of the testicles. And this is precisely the biological purpose. The increased testosterone production provided by the cyst makes the male more masculine and more fertile, which puts him into an ideal position to attract a female, make up for the loss of a mate or a child, and produce new offspring.
NOTE: All organs that derive from the new mesoderm (“surplus group”), including the testicles, show the biological purpose at the end of the healing phase. After the healing process has been completed, the organ or tissue is stronger than before, which allows being better prepared for a conflict of the same kind.
|
If the pressure in a liquid or semi-liquid cyst is too strong, the cyst might burst. A blow against the testicles, exploratory puncture, or premature surgery can cause the rupture. When the cyst breaks, the fluid is released into the testicular sack resulting in the formation of new cysts! Hence, according to Dr. Hamer, the surgical removal of a testicular cyst should only be performed when the cyst is fully matured (indurated).

In men with testicular cancer, a lymphoma or a bone cancer is frequently found in the upper lumbar spine. They are wrongly assumed to be the result of “metastasizing” cells that have traveled there from the testicles. In reality, the enlarged lymph nodes relate to a self-devaluation conflict brought on by
feeling “devalued” as a man, triggered by the cancer diagnosis. The lymphoma develops in the area of the lumbar spine (L2) where the testicles were originally located. If the self-devaluation conflict is experienced as more severe, it affects the lumbar vertebrae.
TESTICLES
|

DEVELOPMENT AND FUNCTION OF THE TUNICA VAGINALIS TESTIS: Starting at the seventh month of gestation, the testicles move from the abdominal cavity through the inguinal canal into the scrotum drawing a portion of peritoneal tissue (abdominal lining) with it as they descend. The inguinal canal closes shortly after birth. The peritoneal layer covering the testicles is known as the tunica vaginalis testis. Its fluid-filled membrane aids the support and protection of the organ. As part of the peritoneum, the tunica vaginalis testis originates from the old mesoderm and is therefore controlled from the cerebellum.
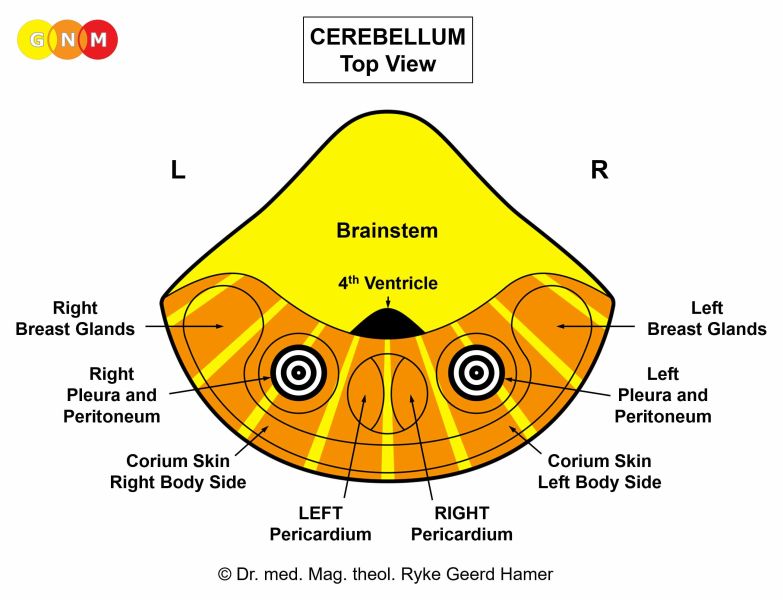
BRAIN LEVEL: In the cerebellum, the tunica vaginalis of the right testicle is controlled from the left side of the cerebellum; the tunica vaginalis of the left testicle is controlled from the right cerebellar hemisphere. Hence, there is a cross-over correlation from the brain to the organ. NOTE: Since the tunica vaginalis was originally part of the peritoneal cavity, the control centers are embedded in the peritoneum relays.
BIOLOGICAL CONFLICT: The biological conflict linked to tunica vaginalis testis is an attack against the testicles. Such an attack conflict might occur in the course of an accident, for example, in sports (hockey, soccer) or with an unexpected kick in the testicles. Verbal threats (“I am going to punch you in the balls!”) could have the same effect. A testicular cancer diagnosis or surgery on the testicles, perceived as an “attack” concerning the integrity of the organ, can also trigger the conflict.
In line with evolutionary reasoning, attack conflicts are the primary conflict theme associated with cerebellum-controlled organs deriving from the old mesoderm.
|
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the tunica vaginalis proliferate. The biological purpose of the cell proliferation is to thicken the peritoneal layer in order to protect the testicle from further attacks. With prolonged conflict activity the additional cells form a lump, considered by conventional medicine as a malignant testicular mesothelioma (see also peritoneal mesothelioma, omental mesothelioma, pleural mesothelioma, and pericardial mesothelioma).
NOTE: Whether the right or left testicle is affected is determined by a man’s handedness and whether the conflict is mother/child or partner-related. A localized conflict affects the “attacked” testicle.
|
HEALING PHASE: Following the conflict resolution (CL), fungi or bacteria such as TB bacteria remove the cells that are no longer required. Healing symptoms are pain because of the swelling and night sweats.

With water retention due to the SYNDROME, additional fluid is stored in the membrane of the tunica causing a so-called hydrocele (“water in the testicles”). However, an injury to the testicles can also cause a hydrocele.
If the inguinal canal does not completely close after birth, fluid accumulated in the peritoneum of the abdominal cavity (see ascites) leaks into the scrotum, resulting in a hydrocele. Also, an inguinal canal that does not close properly leaves a weakened area in the groin, which creates a vulnerability for the development of inguinal hernias (compare with hiatal hernia related to the diaphragm).
NOTE: According to Dr. Hamer, inguinal hernias are not related to a biological conflict. An inguinal hernia showing as a bulge in the groin area (there is one inguinal canal on either side of the lower abdomen) develops due to a weakening of the abdominal muscles caused by pressure in the abdomen from straining or heavy lifting. Women develop hernias after pregnancy or as a result of picking up or carrying a heavy child. In infants, the increased pressure in the abdomen is mainly caused by straining during bowel movements. Hernias in newborns are usually umbilical (navel) hernias.

DEVELOPMENT AND FUNCTION OF THE SMEGMA SECRETING GLANDS: The smegma secreting glands are embedded in the mucous membrane of the inner foreskin that covers the glans penis. The glands secrete a whitish substance (secretory quality) to keep the penis head lubricated during sexual activity (compare with Bartholin’s glands that lubricate the vaginal opening). The smegma secreting glands originate from the endoderm and are controlled from the brainstem.

BRAIN LEVEL: The smegma producing glands are controlled from the left side of the brainstem, next to the control center of the rectum submucosa.
NOTE: The smegma secreting glands, Bartholin’s glands, and bladder submucosa (bladder trigone) share the same brain relay.
BIOLOGICAL CONFLICT: The biological conflict linked to the smegma producing glands is “not being able to penetrate a tight or dry vagina”.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase smegma producing cells proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to improve the smegma production to allow easier penetration.
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer required. Healing symptoms are pain due to the swelling and oozing from the foreskin. If fungi assist healing, this causes “penile candidiasis”. The candidiasis symptoms are already healing symptoms, hence, the condition cannot be contagious (see venereal diseases)!

DEVELOPMENT AND FUNCTION OF THE CORPORA CAVERNOSA: The penis consists of a root, a shaft, and the glans. The corpora cavernosa are two cylinder-shaped chambers that stretch from the pubic bone along the penis shaft to the head of the penis, where they join. They are made of expandable erectile tissue composed mainly of connective tissue. Their core contains a specialized arrangement of blood vessels that fill with blood to achieve an erection. The corpus spongiosum surrounding the penile urethra is for the most part made of smooth muscles (equivalent to the vestibular bulbs of the clitoris). During ejaculation, the muscles contract in a rhythmic movement to allow the expulsion of the ejaculate. The cavernous bodies are enveloped by a dense fibrous sheath, known as the tunica albuginea. The corpora cavernosa originate from the new mesoderm and are therefore controlled from the cerebral medulla.

BRAIN LEVEL: In the cerebral medulla, the right corpus cavernosum is controlled from the left side of the cerebral medulla; the left corpus cavernosum is controlled from the right cerebral hemisphere (in the pelvis relay – see bones). Hence, there is a cross-over correlation from the brain to the organ.
BIOLOGICAL CONFLICT: The biological conflict linked to the corpora cavernosa is a self-devaluation conflict related to the penis brought on, for example, by erection problems after a prostate surgery or due to the adverse effects of testosterone suppressing drugs or antidepressants. Condescending remarks regarding a man’s sexual performance or the size of his penis, not meeting a partner’s sexual expectations, premature ejaculation, and offensive rejections of intercourse or oral sex are other examples of what can make a male feel “worthless there”.
In line with evolutionary reasoning, self-devaluation conflicts are the primary conflict theme associated with cerebral medulla-controlled organs deriving from the new mesoderm.
|
CONFLICT-ACTIVE PHASE: necrosis (cell loss) in the erectile tissue of the penis shaft leading temporarily to an inability to achieve or maintain an erection. For a man unfamiliar with GNM, this typically prompts further penis self-devaluations leading to chronic erectile dysfunction (see also erectile dysfunction related to the penile arteries). The physical impotence does not affect a male’s sex drive since the testosterone level is in the normal range.
NOTE: The penile erection is controlled from the parasympathetic nervous system, ejaculation from the sympathetic nervous system (see male and female orgasm). Hence, the male sex drive is activated in vagotonia. This is why a man cannot have an erection under stress or with intense conflict activity of any biological conflict. The same applies to females (see also vaginal lubrication).
|
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is restored with new cells and the erectile function returns to normal. However, when the healing process is prolonged due to constant conflict relapses, the excess scar tissue affects eventually the flexibility of the penis.

The accumulation of fibrous plaque and hard lumps in the tunica albuginea, the sheath surrounding the corpora cavernosa, causes a permanent bend of the penis. This condition is termed Peyronie’s disease. If a baby boy is born with a curvature of the penis, this reveals that he (perhaps preferred by his mother or parents to be a “she”) had suffered a penis self-devaluation in the womb.

Phimosis, the inability to fully retract the foreskin over the glans, and frenulum breve, a shortening of the frenulum restricting the movement of the foreskin, relate, in GNM terms, to self-devaluation conflicts experienced as “I am worthless there!”
The connective tissue of the foreskin and of the frenulum derives from the new mesoderm and is controlled from the same area in the cerebral medulla as the corpora cavernosa.
Genital warts relate to a sexual separation conflict involving the epidermis of the penis.

DEVELOPMENT AND FUNCTION OF THE GLANS PENIS: The glans penis forms the bulbous-shaped head of the penis shaft. The foreskin covering the glans is a retractable double layer of epidermal tissue enfolding the glans. The foreskin is continuous with the penis skin. The inner foreskin contains smegma secreting glands. The frenulum on the underside of the penis is a small elastic band that allows pulling the foreskin over the glans to protect the urethral opening at the tip of the penis. The glans penis consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex. NOTE: The glans penis is covered by an epidermal skin layer but not endowed with a corium skin (under skin).

BRAIN LEVEL: The glans penis is controlled from the post-sensory cortex (part of the cerebral cortex). The epidermis covering the glans is controlled from the sensory cortex (see brain relays of external genitals).
The right half of the glans penis is controlled from the left side of the post-sensory cortex (between the rectum and right bladder relays); the left half is controlled from the right cortical hemisphere (between the stomach and left bladder relays). Hence, there is a cross-over correlation from the brain to the organ.
NOTE: The glans penis and glans clitoris share the same brain relays. Their control centers are located outside of the temporal lobes; hence, the principle of gender, laterality, and hormone status does not apply.
BIOLOGICAL CONFLICT: The biological conflict linked to the glans penis is a severe separation conflict associated with the penis, experienced, for example, with the loss of a sexual mate or harsh sexual rejection (see also sexual separation conflict related to the epidermis of the penis and scrotum). The conflict also refers to not wanting to be touched at the penis (sexual abuse, sexual molestation, rough handling, unpleasant oral sex, a fear of contracting a venereal disease) or not being allowed to be touched, including touching oneself (a DHS triggered when caught masturbating). The surgical procedure of male circumcision can also prompt a penis conflict.
In line with evolutionary reasoning, territorial conflicts, sexual conflicts, and separation conflicts are the primary conflict themes associated with organs of ectodermal origin, controlled from the sensory, pre-motor sensory and post-sensory cortex.
|
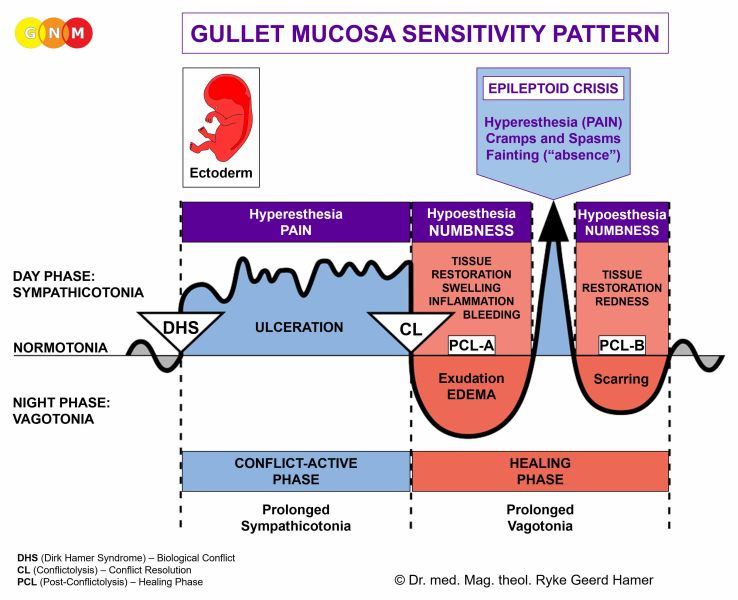 The Biological Special Program of the glans penis follows the GULLET MUCOSA SENSITIVITY PATTERN with hypersensitivity during the conflict-active phase and the Epileptoid Crisis and hyposensitivity in the healing phase.
NOTE: With the exception of the glans penis and glans clitoris, the external genitals follow the Outer Skin Sensitivity Pattern since they are controlled from the sensory cortex.
|
{kind=link}
CONFLICT-ACTIVE PHASE: ulceration (cell loss) in the epithelial lining of the glans. During conflict activity, the penis head is overly sensitive to touch (hypersensitivity).
HEALING PHASE: During the healing phase the ulceration is replenished with new cells. The healing process manifests as hyposensitivity (numbness) of the glans with decreased or, if the conflict was intense, a complete loss of sensitivity. The hypersensitivity is briefly reactivated during the Epileptoid Crisis. With the completion of the Biological Special Program, the penile sensitivity returns to normal.
NOTE: All Epileptoid Crises that are controlled from the sensory, post-sensory, or pre-motor sensory cortex are accompanied by troubled circulation, dizzy spells, short disturbances of consciousness or a complete loss of consciousness (fainting or “absence”), depending on the intensity of the conflict. Another distinctive symptom is a drop of blood sugar caused by the excessive use of glucose by the brain cells (compare with hypoglycemia related to the islet cells of the pancreas).
|
MALE SEXUAL ORGANS - TRANSLATIONS
| ||||||||||