Heart
 DEVELOPMENT AND FUNCTION OF THE MYOCARDIUM (VENTRICULAR HEART MUSCLE): The heart is located in the thoracic cavity in between the lungs. The base of the heart is closely attached to the diaphragm; the pericardium envelops the heart and holds it in place. The coronary arteries and coronary veins supply the heart muscle with blood.
The heart consists of four chambers, the right and left atrium (upper chambers) and the right and left ventricle (lower chambers). The two sides of the heart are separated by the septum. The myocardium is the muscular tissue that makes up the majority of the cardiac wall. It forms the thick middle layer between the epicardium, which is part of the pericardium, and the endocardium that lines the heart cavities and the heart valves. The contractions of the myocardium create the force that initiates the flow of blood through the blood vessels. The two ventricles carry the blood out of the heart. From the right ventricle, oxygen-depleted blood travels through the pulmonary artery to the lungs (pulmonary circulation) while the left ventricle delivers oxygen-rich blood through the aorta to all other organs (systemic circulation). The two atria receive the blood returning to the heart. The right atrium receives deoxygenated blood from the superior and inferior vena cava, the left atrium receives oxygenated blood from the lungs through the pulmonary veins. Continuing the blood flow cycle, the atria empty the blood into the right and left ventricles. Heart valves positioned within the chambers of the heart open and close allowing the blood to flow in one direction.
 This picture shows the two heart tubes of a human embryo before the twist.
In this video, Alexander Tsiaras shares a powerful visualization of the human development from conception to birth.
The AV node (atrioventricular node), situated on the border between the right atrium and right ventricle, picks up the electrical signals for the heartbeat from the sinus node (in the right atrium) and sends them to the bundle of His that carries the cardiac impulse through the bundle branches to the Purkinje fibers. The Purkinje fibers are composed of specialized muscle cells that are able to transmit the electrical discharge more quickly to the ventricles than the other parts of the heart’s conduction system.
The striated muscles of the ventricular myocardium originate from the new mesoderm and are controlled from the cerebral medulla and the motor cortex. The smooth muscles are controlled from the midbrain.
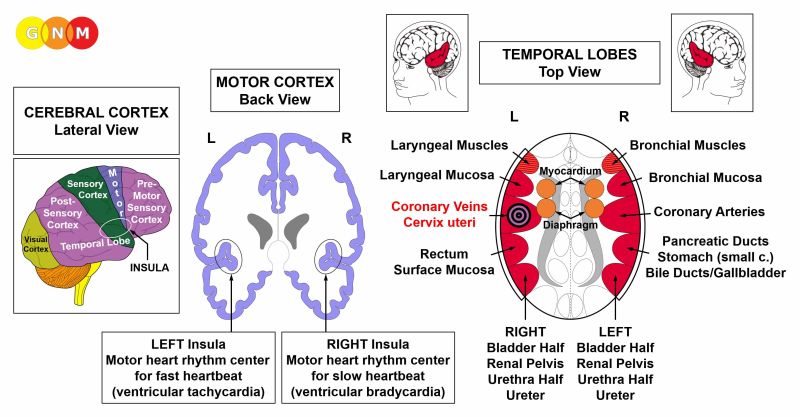
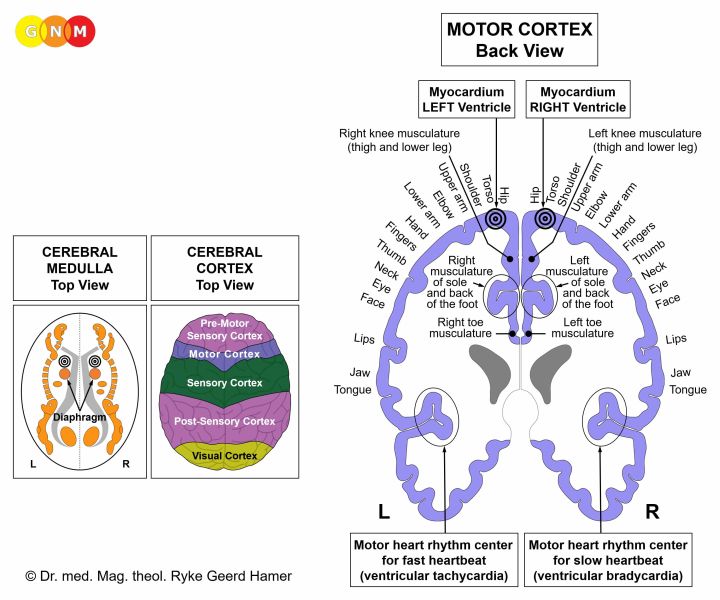 BRAIN LEVEL: The ventricular heart muscle has two control centers in the cerebrum. The trophic function of the muscle, responsible for the nutrition of the tissue, is controlled from the cerebral medulla; the contraction of the muscle and the ventricular conducting system (AV node, bundle branches, Purkinje fibers) are controlled from the motor cortex (part of the cerebral cortex). The right myocardium is controlled from the right side of the cerebrum; the left myocardium is controlled from the left cerebral hemisphere (see GNM diagram showing the motor homunculus). Because of the 180 degree twist of the heart tubes, there is NO cross-over correlation from the brain to the organ. The motor heart rhythm centers control the slow heartbeat (ventricular bradycardia) and the fast heartbeat (ventricular tachycardia).
NOTE: The ventricular heart muscle is functionally closely tied to the diaphragm. The control centers are therefore located right above the brain relays of the diaphragm.
BIOLOGICAL CONFLICT: The biological conflict linked to the ventricular myocardium is an overwhelmed conflict brought on by negative stress overload (compare with physically overwhelmed conflict related to the diaphragm).
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of heart muscle tissue (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing paralysis of the heart muscle (controlled from the motor cortex).
The necrosis takes place on the outside of the myocardium, in the middle, in the inside, or “transmural” (affecting all layers). The loss of cardiac muscle tissue slows the conduction of the heart’s electrical impulses since the signal of the AV node has to circumvent the necrotized area. This causes irregular heartbeats (compare with bradycardial arrhythmia and tachycardial arrhythmia). The condition is called a “bundle branch block” (compare with AV block). If the conflict persists, the thin myocardial wall might rupture with blood flowing into the pericardium (see transudative pericardial effusion). A myocardial perforation could also occur during the Epileptoid Crisis. The rupture causes a cardiac arrest (compare with cardiac arrest related to the pericardium or the coronary arteries).
With lasting conflict activity, the heart muscle becomes weak resulting in physical weakness (difficulty climbing stairs or walking short distances) because of the reduced ability of the heart to carry sufficient amount of blood into the body’s circulatory system. This is medically termed a myocardial or cardiac insufficiency (colloquially called a “heart failure”). When the left myocardium is affected, the reduced heart muscle contraction slows the blood flow in front of the left heart. This causes a backup of blood into the blood vessels that carry blood to the lungs. The increased pressure in the blood vessels pushes fluid into the lungs causing acute shortness of breath and, with an intense conflict, a lung edema, also called cardiac pulmonary edema (compare with alveolar edema related to the lung alveoli; see also lung edema with mitral valve insufficiency). When the right myocardium is affected, the congestion of blood occurs in front of the left heart. The increased pressure forces fluids out of the blood vessels into the surrounding tissue, resulting in a peripheral edema with swelling, particularly in the ankles, feet and legs (see also peripheral edema related to the leg veins or leg bones). In the conflict-active phase involving the right myocardium the blood pressure is elevated (see right myocardial heart attack).
 This brain CT belongs to a right-handed man who suffered an overwhelmed conflict when his wife left him with their children. The brain scan shows the impact in both myocardium relays in the cerebral medulla (orange arrows – view the GNM diagram) associated with his mother/child and partner side. The scan also shows a Hamer Focus in the brain relay of the coronary arteries (red arrows), which reveals that he experienced at the same time a territorial loss conflict. The uneven, edematous ring indicates that the territorial loss conflict has already been resolved. However, the partly sharp border tells that he has still conflict relapses.
HEALING PHASE: During the first part of the healing phase (PCL-A) the necrosis of the heart muscle is replenished through cell proliferation. In conventional medicine, the “tumor” could be diagnosed as a myocardial sarcoma. With an inflammation the condition is called myocarditis – linked to a self-devaluation conflict associated with the heart (see also endocardium and heart valves).
 In PCL-A, an edema develops in the corresponding brain relay. This CT scan shows such a brain edema in the area of the cerebral medulla that controls the right myocardium (view the GNM diagram).
The paralysis of the heart muscle and the related symptoms (shortness of breath, physical weakness, elevated blood pressure) reaches into PCL-A. Recurring healing phases due to continual conflict relapses cause an enlarged heart (cardiomegaly). Constant physical exertion, for example in sports, can also result in a large heart without an overwhelmed-conflict.
During the EPILEPTOID CRISIS, the brain edema is expelled through a sympathicotonic surge. This is the period when the myocardial heart attack occurs. Like the heart attack related to the coronary arteries, the myocardial infarction is initiated in the brain! Controlled from the motor cortex, the myocardial attack manifests itself as contractions of the heart muscle with painful cramps (“heart epilepsy”). An intense Epileptoid Crisis can trigger a generalized epileptic seizure with convulsions involving the whole body, leading potentially to a wrong diagnosis.
The rapid contractions of the myocardium cause tachycardia, a fast heartbeat, also referred to as heart palpitations or ventricular fibrillation (compare with atrial fibrillation related to the smooth heart muscle and ventricular tachycardia related to the coronary veins). The fast heartbeat serves the purpose to ensure the transportation of blood to and away from the heart. The strong heartbeats are typically felt in the neck area. If the contractions are severe, the heart muscle might tear leading to a cardiac tamponade with blood leaking into the pericardium (see also myocardial perforation in the conflict-active phase). This is usually the case if the heart muscle has already been worn out and scarred due to many conflict relapses. With water retention (the SYNDROME) a rupture is more likely to happen. Under normal circumstances, however, the smooth part of the ventricular muscles (about 5-10%) is able to prevent a rupture.
The myocardium is functionally closely tied to the diaphragm, the chief muscle of respiration (in the brain, the brain relays of the diaphragm are located right underneath the control centers of the myocardium). Hence, the myocardial heart attack is always accompanied by diaphragm cramps and breathing difficulties, notably with a right myocardial heart attack since the wall of the right heart is firmly attached to the diaphragm muscle.
Typically, the Epileptoid Crisis is brought on during periods of rest (in vagotonia), often during sleep. The healing crisis occurs as a single event or appears in sequences (see nighttime coughing fits). In the case of the myocardium, this presents as sleep apnea with episodes of cessation of breathing (lasting from a couple of seconds up to two minutes) generated by the contraction of the diaphragm. In GNM terms, sleep apnea is essentially a series of “mini myocardial attacks” with short diaphragm cramps. Chronic sleep apnea indicates conflict relapses triggered by tracks that were established when the original overwhelmed conflict took place. Dreams can also evoke conflict relapses! Sleep apnea is more likely when the left myocardium is involved because the right half of the diaphragm can’t expand as much since the liver is positioned directly underneath it. NOTE: Sleep apnea also occurs with a physical overwhelmed conflict involving only the diaphragm.
Conventional medicine knows only one type of heart attack. According to the standard theory, an “acute myocardial infarction” (“anterior myocardial infarction” or “posterior myocardial infarction”) is caused by cholesterol plaques or a thrombus in the (anterior or posterior) coronary arteries that presumably block the blood and oxygen supply to the heart muscle, resulting in a heart attack. In spite of the evidence that the majority of people who suffered a myocardial heart attack had no coronary artery occlusion and normal cholesterol levels, the coronary artery obstruction hypothesis still prevails. Based on the science of GNM, the myocardium and coronary arteries originate from different embryonic germ layers, are controlled from different areas of the brain, are linked to different biological conflicts, and cause therefore different types of heart attacks, with very specific – predictable – symptoms.
A characteristic symptom of the myocardial heart attack is an acute change of blood pressure due to the distinctive pathways of the two circulatory systems. The right myocardium initiates the flow of blood to the lungs (pulmonary circulation) while the left myocardium moves blood via the aorta to the rest of the body (systemic circulation). Since the distance of blood traveling from the heart through the entire body is much longer than from the heart to the lungs, the left ventricle requires more initial force (“pressure”) than the right heart muscle. This also explains why the left myocardium is larger.
Right myocardial heart attack: If the heart attack involves the right myocardium (see laterality above), the blood pressure in the left heart chamber increases quickly leading to hypertension. The blood pressure is already elevated in the conflict-active phase and in PCL-A due to the paralysis of the right heart muscle. During the Epileptoid Crisis, the blood pressure rises significantly higher in order to compensate the uncoordinated contractions of the right ventricle. Hence, elevated blood pressure does not cause a heart attack, as claimed, but is instead a vital, compensatory symptom during the right myocardial attack (see also kidney parenchyma with hypertension in the conflict-active phase to sustain the function of the kidneys). In contrast, with a heart attack linked to the coronary arteries, the blood pressure remains in the normal range. NOTE: Sustained elevated blood pressure can distort the muscles of the myocardium where the heart valves are attached.
Left myocardial heart attack: When the left myocardium undergoes the Epileptoid Crisis (see laterality above), the blood pressure in the right heart chamber decreases leading to hypotension (see also hypotension related to the carotid sinus). The low blood pressure causes a poor circulation (paleness, light-headedness) and, in acute cases, a complete collapse of the systemic circulation with acute nausea and a loss of consciousness (compare with “absence” during a heart attack involving the coronary arteries). In order to maintain the cardiac function, the pulse rate accelerates. Typically, the red blood cell count rises (polycythemia) to compensate for the temporary oxygen deficiency (compare with anemia, a low red blood cell count). Because of the drop of blood pressure, the left myocardial heart attack is considerably more dangerous than the right myocardial attack. The decreased blood pressure reduces, on the other hand, the risk of a myocardial rupture when the heart muscle cramps (“heart epilepsy”). This is why perforations during left myocardial heart attacks are rare. The attempt to raise the blood pressure through medication can result in a rupture of the heart muscle and death.
 This brain scan shows a glia-ring in the area of the motor cortex that controls the contractions of the right myocardium (view the GNM diagram).
NOTE: Neuroglia restores the brain relay starting from the periphery. The CT, taken shortly after the myocardial heart attack (Epileptoid Crisis), indicates the beginning of PCL-B.
 On this brain CT, we see the presence of neuroglia in the area of the cerebral medulla that controls the trophic function of the right myocardium (view the GNM diagram). The second part of the healing phase (PCL-B) following the myocardial heart attack is already in a more advanced phase. In conventional medicine, the glia buildup is wrongly assumed to be a “brain tumor”.
Understanding Heart Attacks
 |
 DEVELOPMENT AND FUNCTION OF THE MYOCARDIUM (ATRIAL HEART MUSCLE): The right and left atrium constitute the two upper heart chambers. The right atrium receives oxygen-depleted blood from the superior and inferior vena cava; the left atrium receives oxygen-rich blood from the lungs through the pulmonary veins. The atria empty the blood into the right and left ventricles that carry the blood through the pulmonary artery (pulmonary circulation) to the lungs and through the aorta to all other organs (systemic circulation).
The atrial wall consists of smooth muscles (in comparison, the ventricular wall is mainly composed of striated muscles). Like the intestinal muscles that move the “food morsel” along the intestinal canal through peristaltic motion, the smooth heart muscle continually contracts in order to move the “blood morsel” to the ventricles. The rhythmic contraction of the atrial heart muscle is stimulated by the sinus node (sinoatrial node or SA node) located in the upper portion of the right atrium. The sinus node generates an electrical impulse that initiates the heartbeat and sets the rhythm of the pulse (around 50 to 90 times per minute at rest). From there, the electrical signal reaches the AV node and the bundle of His which carry the cardiac impulse through the bundle branches to the ventricles. The heart rate is also determined by the autonomic nervous system: The sympathetic nerves accelerate the heart rate, for example, during excitement and stress as well as during conflict activity and the Epileptoid Crisis (in sympathicotonia); the parasympathetic nerves slow the pulse during rest and sleep (in vagotonia). The sympathetic and parasympathetic nerves meet at the sinus node where they influence the frequency of the heartbeat. The smooth muscles of the atria originate from the endoderm and are controlled from the midbrain.
 BRAIN LEVEL: The smooth muscles of the atrial myocardium are controlled from the midbrain, located at the outermost part of the brainstem.
 The sinus node in the right atrium (previous left heart tube) is controlled from the left side of the brainstem; the sinus node in the left atrium (previous right heart tube) is controlled from the right brainstem hemisphere. NOTE: Because of the 180 degree twist of the embryonic heart tubes, there is a cross-over correlation from the brain to the organ.
An ectopic heartbeat (premature atrial contraction) arises in the right sinus node relay; atrial fibrillation arises in left sinus node relay.
BIOLOGICAL CONFLICT: The biological conflict linked to the atrial myocardium is “not being able to move the blood (morsel)”. The conflict relates to the biological distress that the heart is unable to manage the blood flow and to supply the organism with sufficient amount of blood.
The conflict is usually brought on by a diagnosis such as “your blood flow is poor”, “your arteries are clogged”, “your carotid artery is blocked”, or the scare of a heart attack or stroke, including self-inflicted fears (a “family history of heart diseases”). Taking “blood thinners” can keep the conflict active!
CONFLICT-ACTIVE PHASE: hypertonus of the atrial muscles. The biological purpose of the increased muscle tension is to improve the blood circulation.
HEALING PHASE: During the healing phase the muscle tension goes back to normal. The Epileptoid Crisis manifests as augmented peristalsis of the heart muscle causing atrial fibrillation with tachycardia, an accelerated heartbeat (compare with ventricular fibrillation related to the ventricles and tachycardia during a lung embolism involving the coronary veins). Recurring episodes occur with every conflict relapse. With the completion of the healing phase, the heart rate goes back to normal.
An artificial pacemaker designed to stabilize the heart rate by taking over the job of sending out electrical impulses is, according to Dr. Hamer, only useful when the pacemaker activates both the sinus node and AV node since the two electrical relay stations work together. If, however, the irregular heartbeat originates in the bradycardial or tachycardial heart rhythm center (see coronary arteries and coronary veins), then it is sufficient to stimulate only the AV node.
|
 DEVELOPMENT AND FUNCTION OF THE ENDOCARDIUM AND HEART VALVES: The endocardium is the innermost layer of the myocardium, lining the heart cavities. The myocardium contains four valves that direct the blood flow in one direction. The heart valves are vital to the efficiency of the circulatory systems. The tricuspid valve, located between the right atrium and the right ventricle, opens to empty oxygen-depleted blood into the right ventricle. When the right ventricle contracts, the pulmonary valve opens to deliver the blood into the pulmonary artery that carries the blood to the lungs where it picks up oxygen (pulmonary circulation). Oxygenated blood returning to the heart enters the left atrium where it is stored until the left atrium contracts. At this point, the mitral valve opens allowing the blood to enter the left ventricle. With the contraction of the left ventricle, the aortic valve opens to deliver the blood into the aorta from where it is distributed to the body’s blood vessels (systemic circulation). The endocardium and the heart valves are made of connective tissue, originate from the new mesoderm and are therefore controlled from the cerebral medulla.
 BRAIN LEVEL: In the cerebral medulla, the right endocardium as well as the tricuspid valve and pulmonary valve, located in the right myocardium, are controlled from the right side of the brain; the left endocardium as well as the mitral valve and the aortic valve, located in the left myocardium, are controlled from the left cerebral hemisphere. NOTE: Because of the 180 degree twist of the embryonic heart tubes, there is no cross-over correlation from the brain to the organ.
BIOLOGICAL CONFLICT: The biological conflict linked to the endocardium and the heart valves is a self-devaluation conflict associated with the heart (see connective tissue). Persistent angina pectoris, heart arrhythmia, a previous heart attack or the fear of getting a heart attack (because it “runs in the family”), the diagnosis of a “cardiac insufficiency”, or a doctor’s verdict such as “your heart is weak” or “your heart is not working well” are examples of what can trigger the conflict.
CONFLICT-ACTIVE PHASE: necrosis (cell loss)of the endocardium and/or heart valve(s)
HEALING PHASE: Following the conflict resolution (CL), the tissue loss is refilled and replenished with new cells. If the healing of the endocardium or heart valves is accompanied by an inflammation, this causes endocarditis. Bacteria such as staphylococcus bacteria assist the healing process, provided they are available. Theories that bacteria from an infected tooth or from the throat (“strep throat”) would travel to the heart where they supposedly attach to the heart valves are totally unfounded. In conventional medicine, the symptoms of endocarditis are classified under “rheumatic fever”, even though it is entirely unrelated to rheumatism.
With a hanging healing, that is, when the healing phase is continually interrupted by conflict relapses, the recurring scarification (in PCL-B) eventually impairs the valve(s). Symptoms of valve insufficiencies are heart murmurs.
A mitral insufficiency involves the heart valve situated between the left atrium and the left ventricle. When the mitral valve is affected, the valve does no longer close completely and blood leaks backward through the valve into the pulmonary veins when the heart muscle contracts (such a leakage can also be the result of a progressive necrosis due to a prolonged conflict-active phase). At that point, the condition is irreversible (compare with the distortion of heart valves caused by a pericardial effusion with a restoration of the valve’s function after the healing phase has been completed).
If the scarification thickens the opening of the mitral valve, the orifice becomes narrow and the valve does no longer open fully. This is known as mitral stenosis. A narrowing of the mitral opening compromises the free blood flow from the left atrium to the left ventricle, which increases the diastolic blood pressure (while the systolic blood pressure decreases). The same applies to a tricuspid valve stenosis. At an advanced stage of a mitral valve impairment, surgical procedures might be required in order to prevent a lung edema caused by the congestion of fluids in the lungs (see also lung edema related to the myocardium and alveolar edema related to the lung alveoli).
An aortic insufficiency develops when the aortic valve between the left ventricle and the aorta does no longer close properly due to the scarification. An aortic stenosis occurs when the aortic valve narrows, preventing the valve from opening fully. The obstruction of blood flow impedes the blood flow from the heart into the aorta and to the rest of the body. In this case, the diastolic blood pressure decreases (while the systolic blood pressure increases). The same applies to a pulmonary valve stenosis. Symptoms: dizziness, fatigue, and weakness.
For a person unfamiliar with GNM, the diagnosis of a “heart valve defect” can cause additional self-devaluation conflicts associated with the heart, creating a progressive condition.
|
 DEVELOPMENT AND FUNCTION OF THE PERICARDIUM: The pericardium is a two-layered membrane that envelops and protects the heart. The inner layer (visceral pericardium) is in contact with the heart (epicardium); the outer layer (parietal pericardium) is attached to the sternum and fused to the diaphragm at the base of the heart. Laterally, the pericardium adheres to the pleura. The visceral pericardium is covered by a cell layer called the mesothelium. The mesothelial cells secrete a small amount of serous fluid that fills the space of the pericardial cavity to minimize the friction between the pericardial membranes. In evolutionary terms, the pericardium developed together with the pleura, the peritoneum, and the corium skin. The pericardium originates from the old mesoderm and is therefore controlled from the cerebellum.
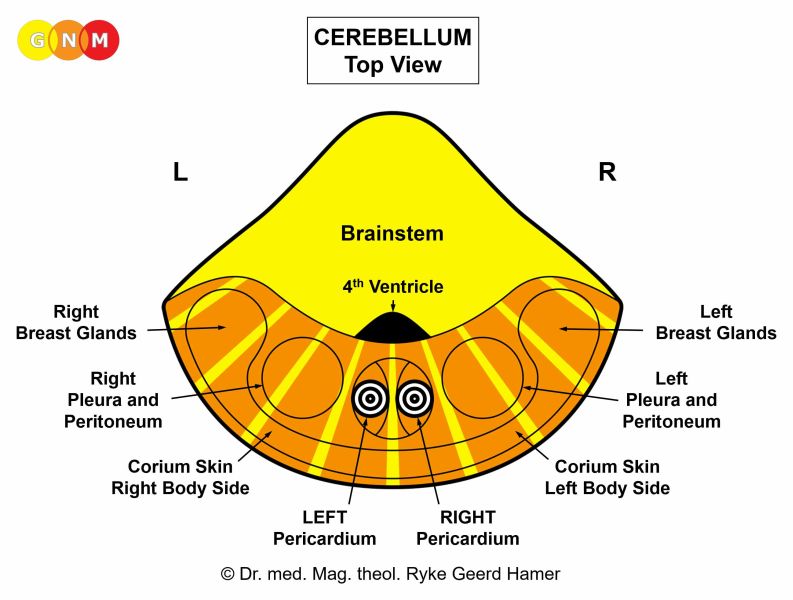 BRAIN LEVEL: In the cerebellum, the right pericardium is controlled from the right side of the brain; the left pericardium is controlled from the left brain hemisphere. NOTE: Because of the 180 degree twist of the embryonic heart tubes, there is no cross-over correlation from the brain to the organ.
BIOLOGICAL CONFLICT: The biological conflict linked to the pericardium is an attack conflict, specifically, an attack against the heart (see also attack conflicts related to the pleura, peritoneum, and corium skin).
An attack against the heart is experienced, for instance, through a stab or blow against the heart or through a push or hit in the upper body during a fight or accident (see also pleura). In a transposed sense, “sharp” words (verbal insults) could be perceived as being “cut to the heart”. Heart surgery such as a bypass operation or a valve replacement might be registered as an assault against the integrity of the organ. In fact, the announcement of a heart surgery and the mental image of being “cut open” can already trigger the conflict. A diagnosis of a “heart disease” or comments of a physician like “your heart is not working properly”, “your ECG results are abnormal”, or “your blood pressure is too high”, associated with a risk of a heart attack, could easily evoke a fear for one’s heart (it might also trigger a self-devaluation conflict affecting the heart valves). The conflict can also be experienced with or on behalf of someone else, let’s say when a loved one suffered a heart attack. Attack conflicts related to the heart also originate inside the chest, for example, with chest pain caused by angina pectoris or during a heart attack.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase pericardial cells proliferate proportionally to the degree and duration of conflict activity. The biological purpose of the cell increase is to create an internal reinforcement to protect the heart against further attacks. With prolonged conflict activity a flat or compact growth develops at the site. In conventional medicine, the thickening of the pericardium is diagnosed as a pericardial mesothelioma (see also pleural mesothelioma, peritoneal mesothelioma, omental mesothelioma, and testicular mesothelioma). Since there are no symptoms during the conflict-active phase, the growth is usually only detected during a routine check-up or follow-up examination.
HEALING PHASE: Following the conflict resolution (CL), fungi, TB bacteria or other bacteria remove the cells that are no longer needed. Healing symptoms are pain behind the sternum caused by the swelling, and night sweats. If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells remain. Eventually, the growth becomes encapsulated.
Pericarditis occurs when healing is accompanied by an inflammation. During the healing phase, the fluid in the pericardium is naturally absorbed by the pericardial membrane (dry pericarditis). Concurrent water retention due to the SYNDROME, however, increases the fluid accumulation (wet pericarditis). Wet pericarditis often develops during hospitalization following a heart surgery.
Excessive water retention brought on, for example, by an existence conflict (the distress during a heart attack) generates an exudative pericardial effusion, a buildup of fluid around the heart. In some people, the pericardium is separated at the midline; the effusion occurs therefore only on the affected side (see also pleural effusion). If the pericardium is not divided, the effusion develops in the entire pericardium (circular pericardial effusion). Only the location of the Hamer Focus in the brain reveals on which side the attack conflict was perceived and therefore from which brain hemisphere the Biological Special Program is directed and controlled.
An acute pericardial effusion could become critical because too much water in the pericardium compresses the heart. Medically, this is termed a cardiac tamponade. The tamponade limits the heart’s normal range of motion leading to severe breathing difficulties, pressure in the chest, and potentially to a cardiac arrest (compare with cardiac arrest related to the myocardium or coronary arteries). This explains why a cardiac tamponade is the most feared complication after a heart attack or following heart surgery.
The pericardial effusion might distort the heart valve(s). However, after healing has been complete the valves regain their normal function (compare with mitral insufficiency where the condition is irreversible).
 This CT scan shows scarification (PCL-B) in the area of the cerebellum that controls the right and left pericardium (view the GNM diagram), which indicates that the attack conflict was associated with the entire heart. However, the Biological Special Program has been completed.
|
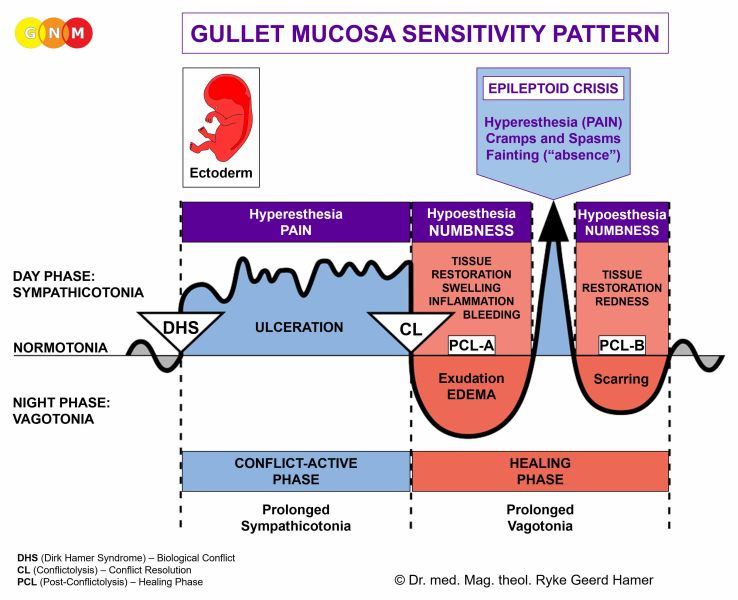
 DEVELOPMENT AND FUNCTION OF THE CORONARY ARTERIES: The coronary arteries and coronary veins run along the outer surface of the heart in a crown-like (“coronary”) shape. Two coronary arteries branch off from the aorta near the top of the heart. Their main function is to deliver oxygen-rich blood to the heart muscle. Contrary to other blood vessels, the inner lining of the coronary arteries, the so-called intima, consists of highly sensitive squamous epithelial cells that originate from the ectoderm and are therefore controlled from the cerebral cortex. The arterial wall is composed of smooth muscles and striated muscles.
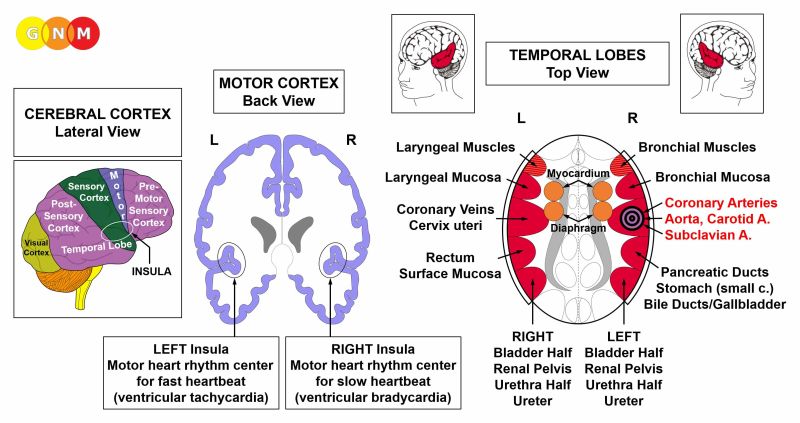 BRAIN LEVEL: The coronary artery intima is controlled from the right insula (part of the temporal lobe). The control center of the coronary arteries is positioned across from the brain relay of the coronary veins.
The trophic relays of the diaphragm and of the myocardium that house the AV-node border on the insula from within.
 The INSULA is located deep in the cerebral cortex, exactly at the point where the four cerebral cortices meet (pre-motor sensory cortex, motor cortex, sensory cortex, post-sensory cortex). It is the area of the brain that controls the lining of the large blood vessels (coronary arteries, coronary veins, aorta, carotid arteries, and subclavian arteries) that deliver blood to and from the heart. The right and left insula also regulate the slow (bradycardial) and fast (tachycardial) heart rate of the ventricles (myocardium) – see AV node. The bradycardial heart rhythm center is located in the right insula; the tachycardial heart rhythm center is located in the left insula. The heart rhythm (slow and fast) constitutes together with the diaphragmatic breathing a superordinate system.
BIOLOGICAL CONFLICT: The biological conflict linked to the coronary arteries is a male territorial loss conflict or a female sexual conflict, depending on a person’s gender, laterality, and hormone status (see also Postmortal Constellation, Casanova Constellation, Nympho Constellation).
A territorial loss conflict is experienced through the loss of the private domain (a home because of an unexpected move or a divorce, the confiscation of a property, fire, flooding) or a threat to the safety of the place where one lives. Assets of the “territory” that are of personal value such as a car, jewelry, a private collection, stocks, investments, a license, an immigrant status, or a club membership also fall into this category. The loss of the professional domain could occur through the loss of a business, bankruptcy, the loss of a workplace because of layoffs, a merger, a transfer, or an early retirement due to illness or cut-backs. Not being able to continue pursuing a hobby (playing a musical instrument, painting, writing, gardening, a sports activity) can be perceived as a territorial loss. The conflict also refers to the loss of the intellectual domain, for instance, to the loss of one’s skills as a result of an accident, or, literally, to the loss of the intellectual property (research results, confidential data, patents, trade secrets). The loss of a member of the territory (parent, spouse, partner, child, a pet, friend, colleague, client, customer) because of an argument or a separation can prompt the conflict. Men suffer territorial loss conflicts when they lose a sexual mate. The male territorial loss conflict is the equivalent to the female sexual conflict (the brain relays of the corresponding organs, namely of the coronary arteries and cervix uteri, are positioned exactly across from each other in the cerebral cortex).
CONFLICT-ACTIVE PHASE: ulceration in the inner lining of the coronary arteries. The biological purpose of the cell loss is to widen the lumen of the coronary vessel so that more blood can flow to the heart. The enhanced energy puts the individual in a better position to get the territory back or establish a new one. The ulceration of the sensitive intima causes angina pectoris (and not, as assumed, a myocardial insufficiency). Depending on the degree of the conflict, the chest pain ranges from mild to severe.
 This brain CT shows the impact of a territorial loss conflict in the brain relay of the coronary arteries (view the GNM diagram). The sharp border of the Hamer Focus reveals that the person is conflict active.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation with swelling due to the edema (fluid accumulation). The swelling might temporarily occlude the affected artery, particularly with concurrent water retention (the SYNDROME). However, a narrowing (stenosis) of the coronary vessel can never lead to a heart attack because, should the situation of an occlusion arise, auxiliary vessels or so-called collaterals act as a natural bypass to supply the heart with blood (the collaterals are like a dry river bed, so to speak, that are filled with blood within 2-3 days after a coronary blockage. In embryological terms, the collateral blood vessels originate from the new mesoderm). This clearly refutes the standard theory claiming that a heart attack is caused by a coronary artery obstruction. It also questions the need for bypass operations or angioplasty.
The lining of the coronary arteries is restored predominantly with the help of cholesterol. Hence, during the healing phase, the cholesterol level rises. With a hanging healing, that is, when the healing process is continually interrupted by conflict relapses, the buildup of cholesterol plaques leads to atherosclerosis and, eventually, to a narrowing of the lumen of the blood vessel. Over time, the arterial wall hardens and loses its elasticity, a condition known as arteriosclerosis (see also atherosclerosis related to the aorta, carotid arteries, subclavian arteries, and other blood vessels).
Cholesterol is mainly produced in the liver. In fact, 80% of the total cholesterol is synthesized within the body; only 20% comes from dietary sources. The liver uses fats from foods as raw material to manufacture cholesterol. The so-called LDL-cholesterol, labeled as the “bad cholesterol”, is particularly useful as it is very sticky and therefore ideal for repairing the blood vessel wall. Cholesterol-lowering medication such as statin drugs suppresses the liver’s cholesterol production. This is why statin drugs have a negative effect on the liver. Statin drugs also damage muscle tissue, including the heart muscle, which is detrimental for the overall function of the heart.
The EPILEPTOID CRISIS is the moment when the heart attack occurs. Contrary to the standard belief, the heart attack is not caused by an occlusion of a coronary artery but initiated in the brain, precisely, when the brain edema that developed in PCL-A is expelled through a sympathicotonic surge triggered by a brief, pre-programmed reactivation of the conflict (see also heart attack related to the myocardium). From a biological point of view, the heart attack is crucial, since the heart can only resume its normal function after the brain edema has been pressed out.
The heart attack linked to the coronary arteries presents as acute angina pectoris with strong pain behind the sternum. The pain might radiate into the left shoulder and left arm. Accompanying symptoms are cold sweats and nausea. Since the striated muscles of the coronary artery wall undergo the Epileptoid Crisis at the same time, heart vessel spasms occur together with the angina pain. These muscle cramps are entirely unrelated to the myocardium, which is controlled from a different part of the brain and linked to an overwhelmed conflict. During the contractions of the coronary artery muscles, cholesterol plaques from the intima might become loose and get carried into the bloodstream, where they are washed out in the normal course of blood flow (compare with lung embolism).
The real danger of the heart attack is the involvement of the bradycardial heart rhythm center. Normally, the heart beats in a regular, balanced rhythm. This, however, changes for the duration of the Epileptoid Crisis when the brain edema in the coronary arteries relay is expelled. The pressure created by the momentary sympathicotonic surge slows the pulse, causing bradycardia (compare with tachycardia related to the coronary veins; see also bradycardia related to the carotid sinus). Recurring episodes of bradycardial arrhythmia are triggered by conflict relapses.
With a very intense Epileptoid Crisis due to a large brain edema the heartbeat could come to a complete stop, or cardiac arrest (compare with cardiac arrest related to the myocardium or the pericardium).
In conventional medicine, bradycardia is thought to be caused by a blockage of the electrical conduction system at the AV node and therefore referred to as an atrioventricular block or AV block (compare with “bundle branch block”). Dr. Hamer's research, however, shows that the function of the AV node is only to transfer the electrical impulses from the sinus node to the ventricles, while the synchronization of the heartbeats is coordinated and controlled from the bradycardial and tachycardial heart rhythm centers located in the insula of the cerebral cortex (see brain relays of the coronary arteries and coronary veins).
 This CT scan shows a brain edema (fluid accumulation) in the control center of the coronary arteries (view the GNM diagram). The edema developed after the territorial loss conflict was resolved (in PCL-A). Water retention due to the SYNDROME enlarges the edema considerably.
NOTE: A large brain edema in this part of the cerebrum might press onto the motor cortex, specifically during the Epileptoid Crisis when the actual heart attack occurs. The involvement of the motor cortex results in a temporary paralysis on the left side of the body (see red stroke). In conventional medicine, the dark (hypodense) area on the brain scan is interpreted as a “brain infarction”, believed to be caused by a blockage of a cerebral artery (see collaterals ensuring the cerebral blood flow).
 The glia-ring in the coronary arteries relay (view the GNM diagram) indicates the beginning of PCL-B. The brain scan was taken shortly after the expected heart attack.
In conventional medicine, the presence of glia is diagnosed as a “brain tumor”, precisely, as a high-grade glioma (glioblastoma) “white on the outside and necrosis in the middle”. The brain CT, however, demonstrates that neuroglia (brain connective tissue) starts restoring the brain relay from the periphery! This is in clear contradiction to the established theory that a cancer, including a “brain cancer”, grows through continued cell augmentation leading to the formation of a tumor.
 Based on the established “brain tumor” theory, conventional medicine classifies the white (hyperdense) area as a “grade 4 glioma” with a poor prognosis. According to Dr. Hamer's research, the buildup of neuroglia is a positive sign that the healing process in the coronary arteries (view the GNM diagram) is almost complete.
|

 DEVELOPMENT AND FUNCTION OF THE CORONARY VEINS: The coronary arteries and coronary veins run along the outer surface of the heart. The coronary veins receive oxygen-depleted blood from the heart muscle and empty it into the right atrium from where it passes to the right ventricle and further into the lung artery and the lungs, where the blood picks up fresh oxygen (pulmonary circulation). The pulmonary artery is unique insofar as it is the only artery in the human body that carries de-oxygenated blood. Contrary to other blood vessels, the inner lining of the coronary veins, the so-called intima, consists of highly sensitive squamous epithelial cells that originate from the ectoderm and are therefore controlled from the cerebral cortex. The wall of the coronary veins is composed of smooth muscle and striated muscles.
 BRAIN LEVEL: The coronary vein intima is controlled from the left insula (part of the temporal lobe). The control center of the coronary veins is positioned across from the brain relay of the coronary arteries.
The trophic relays of the diaphragm and of the myocardium that house the AV-node border on the insula from within.
The INSULA is located deep in the cerebral cortex, exactly at the point where the four cerebral cortices meet (pre-motor sensory cortex, motor cortex, sensory cortex, post-sensory cortex). It is the area of the brain that controls the lining of the large blood vessels (coronary arteries, coronary veins, aorta, carotid arteries, and subclavian arteries) that deliver blood to and from the heart. The right and left insula also regulate the slow (bradycardial) and fast (tachycardial) heart rate of the ventricles (myocardium) – see AV node. The tachycardial heart rhythm center is located in the left insula; the bradycardial heart rhythm center in the right insula. The heart rhythm (slow and fast) constitutes together with the diaphragmatic breathing a superordinate system.
BIOLOGICAL CONFLICT: The biological conflict linked to the coronary veins is a female sexual conflict or a male territorial loss conflict, depending on a person’s gender, laterality, and hormone status (see also Postmortal Constellation, Casanova Constellation, Nympho Constellation). In women, a sexual conflict also affects the cervix uteri. NOTE: A male experiences a female sexual conflict when he has a low testosterone status. If his testosterone level is in the normal range, a sexual conflict affects the prostate.
A sexual conflict refers to any distress concerning sexuality. This includes painful (first-time) sex, sexual abuse, sexual harassment, unwanted sexual practices, sexual rejection, feeling sexually unwanted, a lack of sexual activity because of an unexpected separation or loss of a mate. Offensive pornography, finding out that the partner or spouse is sleeping with someone else, or interruptions during sexual intercourse can also trigger the conflict.
CONFLICT-ACTIVE PHASE: ulceration in the lining of the coronary veins proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the lumen of the blood vessel to improve the blood flow. The ulceration of the sensitive intima causes moderate angina pectoris. In females, the cervical lining also ulcerates, which, however, goes unnoticed.
 This CT scan shows the impact of a sexual conflict in the area of the brain that controls the coronary veins (view the GNM diagram). The sharply defined border of the Hamer Focus indicates conflict activity. In females, this also affects the cervix uteri.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation. Like the restoration of the coronary arteries, the repair of the coronary veins is mainly accomplished with the help of cholesterol.
The EPILEPTOID CRISIS presents as a temporary reactivation of angina pectoris with cramp-like chest pain since the striated muscles of the coronary veins are also involved. During the muscle contractions, small pieces of cholesterol plaque are pulled off from the blood vessel wall and are pushed into the lung circulation, where they block the lung artery causing a lung embolism with shortness of breath. Depending on the intensity and duration of the conflict-active phase, the symptoms range from mild to severe.
Conventional medicine claims that a lung embolism is caused by a blood clot that supposedly arises in the lower extremities and travels through the entire venous system, including the heart, all the way to the lungs. In reality, the “pulmonary emboli” are healing scabs originating in the coronary veins. Blood-thinning medication taken at that point to “reduce blood clotting” might contribute to acute bleeding from the cervix that undergoes the Epileptoid Crisis at the same time.
The real danger of the lung embolism is the involvement of the tachycardial heart rhythm center. Normally, the heart beats in a regular, balanced rhythm. This, however, changes for the duration of the Epileptoid Crisis when the brain edema in the coronary vein relay is expelled. The pressure created by the momentary sympathicotonic surge accelerates the pulse, causing tachycardia (compare with bradycardia, a slow heartbeat, related to the coronary arteries; see also ventricular tachycardia and atrial tachycardia). Recurring episodes of tachycardial arrhythmia combined with rapid breathing (tachypnea) or gasping for breath are triggered by conflict relapses. Permanent tachycardial arrhythmia, however, can cause death since the incessant fluttering heartbeats eventually stop the blood flow (hemodynamic stasis).
 The accumulation of neuroglia in the brain relay of the coronary veins (view the GNM diagram) indicates that the person has already passed the Epileptoid Crisis (lung embolism) and is now in the second part of the healing phase (in PCL-B). In conventional medicine, the glia buildup is wrongly assumed to be a “brain tumor”.
|
 DEVELOPMENT AND FUNCTION OF THE AORTA, CAROTID ARTERIES, AND SUBCLAVIAN ARTERIES: The aorta is the main artery of the body. The aorta arises at the pericardium directly after the aortic valve where it takes the blood from the left ventricle and distributes it to the rest of the body (systemic circulation). Anatomically, the aorta is a tube that extends from the heart upward (ascending aorta), curves over the heart (aortic arch) and continues downward through the chest (descending aorta). There it subdivides into the thoracic aorta and abdominal aorta. The two common carotid arteries that run along both sides of the head and neck divide into the internal and external carotid arteries. The internal carotid arteries carry blood from the heart to the brain; the external carotid arteries deliver blood to the face and the scalp. The cerebral arteries branch off the internal carotid artery. The subclavian arteries are paired arteries below the collarbones that supply the arms with blood. The left subclavian artery arises from the aortic arch; the right subclavian artery arises with the right common carotid artery from the brachiocephalic trunk, or brachiocephalic artery, that supplies blood to the right arm, head and neck. The vertebral arteries arise from the respective subclavian artery. Contrary to other blood vessels, the inner lining of the ascending aorta, the common carotid arteries, the internal carotid arteries, and the inner sections of the subclavian arteries consist of squamous epithelium, originate from the ectoderm and are, therefore, controlled from the cerebral cortex. The arterial wall is composed of smooth muscles and striated muscles.
BRAIN LEVEL: The squamous epithelial lining of the ascending aorta, internal carotid arteries, and inner sections of the subclavian arteries is controlled from the right insula (part of the temporal lobe). Their control center is positioned across from the brain relay of the coronary veins.
The insula is located deep in the cerebral cortex, exactly at the point where the four cerebral cortices meet (pre-motor sensory cortex, motor cortex, sensory cortex, post-sensory cortex).
BIOLOGICAL CONFLICT: a male territorial loss conflict or a female sexual conflict, depending on a person’s gender, laterality, and hormone status (see coronary arteries)
CONFLICT-ACTIVE PHASE: ulceration in the affected artery proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the lumen of the arterial vessel to improve the blood flow. Symptoms: pain ranging from mild to severe. NOTE: While conflict active, the person is in a depressed mood.
If the conflict persists, the blood vessel wall becomes weak causing a localized bulge at the ulcerated area. This is called an aortic aneurysm, carotid artery aneurysm or subclavian artery aneurysm (compare with abdominal aortic aneurysm and aneurysms related to the external carotid artery, the outer sections of the subclavian arteries, or cerebral aneurysm). Small aneurysms may go completely unnoticed. However, as the aneurysm increases in size, there is a greater risk of rupture with bleeding into the surrounding tissue and potentially serious complications. Normally, the smooth muscle fibers embedded in the striated muscles of the arterial wall stabilize the blood vessel to prevent a rupture. An aneurysm rupture therefore only occurs because of a vigorous move or heavy lifting.
HEALING PHASE: During the first part of the healing phase (PCL-A), the tissue loss is replenished through cell proliferation with swelling due to the edema (fluid accumulation) in the healing area. The blood vessel wall is repaired mainly with calcium and cholesterol. With a hanging healing, that is, when the healing process is continually interrupted by conflict relapses, the buildup of cholesterol deposits eventually leads to atherosclerosis (see also atherosclerosis related to the coronary arteries and other blood vessels). A large swelling, usually because of concurrent water retention due to the SYNDROME, and the accumulation of atherosclerotic plaques can lead to a narrowing of the artery with dizziness and fainting if the carotid artery is affected (carotid artery stenosis).
During the muscle contractions that take place in the arterial wall throughout the Epileptoid Crisis, small pieces of cholesterol plaque (erroneously believed to be a “thrombus”) might break off and travel to the brain. However, a blockage of the carotid artery does not cause a stroke, as claimed by conventional medicine. As is the case with an occlusion of the coronary arteries, should the situation of an obstruction arise, auxiliary vessels or so-called collaterals act as a natural bypass to supply the brain with blood and oxygen.
|
 DEVELOPMENT AND FUNCTION OF THE CAROTID SINUS: The carotid sinus is a bulbous area, located bilaterally (on both sides of the neck) close to the point where the carotid arteries bifurcate. The carotid sinus contains pressure receptors that control the body’s blood pressure by mediating changes in the heart rate. The lining of the carotid sinus consists of squamous epithelium, originates from the ectoderm and is therefore controlled from the cerebral cortex.
 BRAIN LEVEL: The carotid sinus is controlled from the right insula (part of the temporal lobe). The insula is located deep in the cerebral cortex, exactly at the point where the four cerebral cortices meet (pre-motor sensory cortex, motor cortex, sensory cortex, post-sensory cortex). Their control center is positioned across from the brain relay of the coronary veins.
NOTE: The carotid sinus, coronary arteries, ascending aorta, internal carotid arteries, and inner sections of the subclavian arteries share the same control center.
BIOLOGICAL CONFLICT: the blood pressure is too high
CONFLICT-ACTIVE PHASE: ulceration in the carotid sinus proportional to the degree and duration of conflict activity. The biological purpose of cell loss is to lower the blood pressure. Continuous, intense conflict activity causes carotid sinus hypersensitivity with marked bradycardia (compare with slow heartbeat during the coronary arteries-related heart attack) and a drop of blood pressure (compare with drop of blood pressure during the left myocardial heart attack).
HEALING PHASE: During the first part of the healing phase (PCL-A) the ulcerated area is replenished through cell proliferation. The carotid bulb is repaired predominantly with cholesterol. With a hanging healing the accumulation of cholesterol plaque, called a carotid bifurcation atheroma, narrows the lumen of the carotid artery (compare with carotid artery stenosis causing dizziness and lightheadedness but NOT a stroke; see cerebral collateral circulation in carotid artery disease).
| ||||||||||||