Brain
 DEVELOPMENT AND FUNCTION OF THE PITUITARY GLAND: The pituitary gland, or hypophysis, is an endocrine gland (see also pineal gland, or epiphysis) situated at the base of the brain in the sella turcica, a saddle-shaped depression in the sphenoid bone. It is a protrusion off the bottom of the hypothalamus. The adenohypophysis (anterior lobe) secretes hormones (secretory quality) responsible for physical growth (growth hormone STH-Somatotropin Hormone), reproduction (LH-Luteinizing Hormone promotes ovulation; FSH-Follicle Stimulating Hormone plays a role in pubertal development), metabolism (TSH-thyroid stimulating hormone), cortisol levels (ACTH-adrenocorticotropic hormone) and some aspects of pregnancy, childbirth (oxytocin induces the contraction of the uterus muscles during labor) and lactation (prolactin stimulates the breast glands to produce milk). The adenohypophysis consists of intestinal cylinder epithelium, originates from the endoderm and is therefore controlled from the brainstem. The neurohypophysis (posterior lobe) is of ectodermal origin (to date, the related biological conflict is unknown).
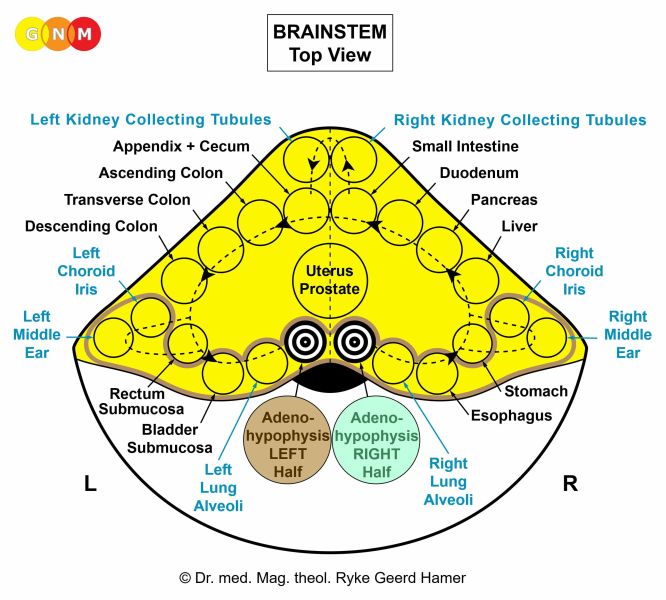 BRAIN LEVEL: In the brainstem, the adenohypophysis has two control centers, positioned within the ring form of the brain relays that control the organs of the alimentary canal.
The right half of the adenohypophysis is controlled from the right side of the brainstem; the left half is controlled from the left brainstem hemisphere. There is no cross-over correlation from the brain to the organ.
NOTE: The mouth and pharynx, tear glands, Eustachian tubes, thyroid gland, parathyroid glands, pituitary gland (adenohypophysis), pineal gland, and choroid plexuses share the same brain relays.
STH-PRODUCING CELLS
BIOLOGICAL CONFLICT: The biological conflict linked to the STH (Somatotropin Hormone) producing cells of the adenohypophysis is a morsel conflict.
RIGHT HALF of the adenohypophysis: Equivalent to the right half of the mouth and pharynx, the right half of the adenohypophysis correlates to an “ingoing morsel” and to “not being able to grab a morsel because the individual is too small”. Example: a young child is competing with an adult or a bigger child, let’s say, in sports such as soccer.
LEFT HALF of the adenohypophysis: Equivalent to the left half of the mouth and pharynx, the left half of the adenohypophysis correlates to an “outgoing morsel” and to “not being able to get rid of a morsel because the individual is too small” (originally, the feces morsel). Example: a child or adolescent has to take over a parent’s role.
In general, the conflict is brought on by feeling “too little” (provoked, for instance, by comments of a parent, teacher, or coach). The distress of being “too small” can also occur in adults.
CONFLICT-ACTIVE PHASE: During the conflict-active phase, the STH producing cells proliferate proportionally to the intensity of the conflict. The biological purpose of the additional cells is to increase the production of growth hormones to put the individual into a better position to grab (right half) or get rid of a morsel (left half). With prolonged conflict activity a compact tumor (secretory type) forms as a result of the continuous cell augmentation. In conventional medicine, a tumor in the adenohypophysis is called a pituitary adenoma (generally considered as “benign”).
In children and adolescents, the overproduction of growth hormones leads to real, potentially excessive physical growth (gigantism). If the conflict happens in adulthood the increased hormone production causes enlarged hands, feet, and facial feature (acromegaly). When the left half of the adenohypophysis is affected, the lips also enlarge (the gullet opening becomes larger so that the morsel can be better expelled).
 Maurice Tillet (1903-1954), a French professional wrestler, developed acromegaly in his twenties.
At the age of 13, Maurice still had a normal stature.
HEALING PHASE: In the healing phase, fungi or mycobacteria such as TB bacteria remove the cells that are no longer required. The healing process is accompanied by night sweats.
If healing cannot be completed (hanging healing) because of recurring conflict relapses, more and more adenohypophysis tissue is lost leading to a decrease or complete cessation of STH-Somatotropin Hormone production. During the development of a child, this results in a short stature (dwarfism).
PROLACTIN PRODUCING CELLS
BIOLOGICAL CONFLICT: The biological conflict linked to the prolactin-producing cells is a feeding conflict as in “not being able to nourish the child or the family”, let’s say, because of financial difficulties (e.g., unemployed or self-employed single mothers). The conflict can affect either of the two halves of the gland.
CONFLICT-ACTIVE PHASE: During the conflict-active phase, the prolactin-producing cells in the pituitary gland proliferate proportionally to the intensity of the conflict. The biological purpose of the additional cells is to increase the secretion of prolactin to be better able to nurse the child or the family. With lasting conflict activity the additional cells form a compact growth (secretory type). In conventional medicine, the tumor is termed a “secretory pituitary adenoma” or prolactinoma. The overproduction of prolactin causes an increased milk production if a woman is breastfeeding at the time of conflict activity. However, even if a woman is not nursing, the increase of prolactin still results in a secretion of milk, noticeable as a milky nipple discharge or spontaneous flow of milk from the breasts. Lactation also occurs in males who suffered a feeding conflict (see also breast cancer in men). In both sexes the condition is called galactorrhea.
HEALING PHASE: With a prolonged healing phase more and more glandular tissue gets lost as a result of the continuous cell removal process. In nursing females, this causes a reduced or complete stop of milk production. If this happens during pregnancy, a woman has little or no breast milk after the birth of her child (compare with lack of milk production related to the breast glands).
LH and FSH PRODUCING CELLS
BIOLOGICAL CONFLICT: The biological conflict linked to the luteinizing hormone (LH) and follicle stimulating hormone (FSH) producing cells of the adenohypophysis is “being too immature”, literally or figuratively, with an overproduction of LH and FSH in the conflict-active phase. The conflict occurs before puberty. In children, continuous conflict activity leads to a premature development (precocious puberty). A long-lasting healing phase causes a decrease of LH and FSH production resulting in delayed puberty (no breast and ovary development in girls by the age of 13 or growth of testes in boys by the age of 14).
 This brain CT shows calcification (upper arrows) in the adenohypophysis (compare with calcification in the pineal gland and choroid plexus). The scarring in the brain relays that control the adenohypophysis (lower arrows – view the GNM diagram) confirms that the healing phase has been completed.
NOTE: The adenohypophysis is located close to the optic chiasm. Hence, a large pituitary adenoma (usually because of water retention due to the SYNDROME) might compress the optic nerve causing temporary vision impairment; damage to the optic nerve can result in blindness.
|
 DEVELOPMENT AND FUNCTION OF THE PINEAL GLAND: The pineal gland (epiphysis) is a small endocrine gland located deep in the center of the brain behind the third ventricle, precisely, in the groove where the two halves of the thalamus join (compare with pituitary gland, or hypophysis). The pineal gland is comprised of pineal cells (pinealocytes) that register the incidence of light (absorptive quality) and produce melatonin (secretory quality). Melatonin (not to be confused with the pigment melanin) plays an important role in regulating the night-day cycle in synchronization with the sleep-wake cycle (circadian rhythm). The pineal gland consists of intestinal cylinder epithelium, originates from the endoderm and is therefore controlled from the brainstem.
 BRAIN LEVEL: In the brainstem, the pineal gland has two control centers positioned within the ring form of the brain relays that control the organs of the alimentary canal.
The right half of the pineal gland is controlled from the right side of the brainstem; the left half is controlled from the left brainstem hemisphere. There is no cross-over correlation from the brain to the organ.
NOTE: The mouth and pharynx, tear glands, Eustachian tubes, thyroid gland, parathyroid glands, pituitary gland, pineal gland, and choroid plexuses share the same brain relays.
BIOLOGICAL CONFLICT: The biological conflict associated with the pineal gland is linked to sudden long darkness (compare with light-related conflict linked to the pupil muscles). The right half of the pineal gland correlates to “not being able to capture light”, whereas the left half of the pineal gland corresponds to “not being able to get rid of darkness”. The conflict is brought on, for instance, by distress experienced in dark places (basement, underground mines or caves, tunnels) or, figuratively, through being kept “in the dark”.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the pineal gland proliferate proportionally to the intensity of the conflict. The biological purpose of the additional cells is to increase the production of melatonin in order to increase the reception of light. With prolonged conflict activity a compact (secretory type) or flat growing tumor (absorptive type) forms as a result of the continuous cell augmentation. The medical term for a pineal tumor is “pinealoma” or “pineal ependymoma”. A large growth might constrict the oculomotor nerve (third cranial nerve) that supplies the majority of the extraocular muscles controlling eye movements. Damage to the nerve leads to an inability to move the affected eye normally (see strabismus). When a pineal tumor compresses the third ventricle, this causes a hydrocephalus.
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. The healing process is accompanied by night sweats. During the decomposing process the tumor might bleed. The bleeding occurs when the outer wall of the tumor breaks (compare with brain bleeding due to the rupture of a brain cyst).
 This brain scan was taken after a pineal tumor was removed with the help of TB bacteria. The caverns that are created after the tumor has been decomposed are filled with calcium. Here already visible as white specks. Tiny calcified structures in the pineal gland, indicating a short healing phase, are known as corpora arenacea, or brain sand.
 This brain CT shows the completion of the calcification process (compare with calcification in the pituitary gland and choroid plexus).
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the tumor cannot be broken down and therefore remains. Eventually, the growth becomes encapsulated. A pineal cyst is an encapsulated pineal tumor containing fluid due to water retention.
|
 DEVELOPMENT AND FUNCTION OF THE THALAMUS AND HYPOTHALAMUS: The thalamus and hypothalamus are situated deep in the brain between the cerebral cortex and the midbrain. They form the larger part of the diencephalon (interbrain). The two halves of the thalamus are located symmetrically on each side of the third ventricle. The hypothalamus is located below the thalamus. The hypothalamus is the coordinating center of the autonomic nervous system and the endocrine system, affecting sleep rhythm, metabolic functions, intake of food and water (hunger, thirst), body temperature, and the release of hormones from the pituitary gland. The thalamus and hypothalamus originate from the ectoderm and are controlled from the diencephalon.
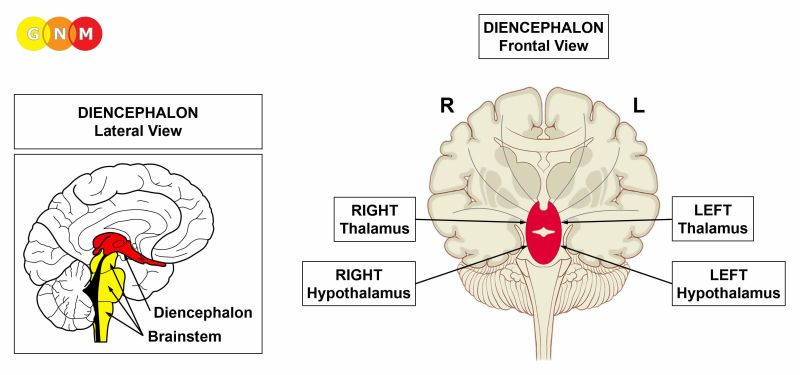 BRAIN LEVEL: The thalamus and hypothalamus are controlled from the diencephalon (interbrain), which is located in the central part of the cerebrum just above the midbrain. The right thalami are controlled from the right side of the diencephalon; the left thalami from the left side. There is no cross-over correlation from the brain to the organ. NOTE: In case of the thalamus and hypothalamus, the organs and their control centers are in the same location (compare with pituitary gland and pineal gland that are situated in the center of the brain but are controlled from the brainstem).
BIOLOGICAL CONFLICT: complete self-abandonment; complete resignation (“I wish I were dead“)
CONFLICT-ACTIVE PHASE: change of hormonal parameters and activation of the autonomic nervous system (sympathicotonia) in order to be able to manage the stress. Symptoms: wakefulness and extreme restlessness.
HEALING PHASE: In the course of the healing phase the hormonal parameters normalize and the nervous system switches into vagotonia.
With the SYNDROME, that is, with water retention as a result of an active abandonment or existence conflict, there is a risk that a large brain edema (PCL-A) compresses the third ventricle (see hydrocephalus); even more so, when both halves of the thalamus undergo the healing process at the same time.
 This MRI taken with contrast substance shows a healing process in the area of the brain that controls the left thalamus (view the GNM diagram). In conventional medicine, the “mass” is erroneously diagnosed as a “brain tumor” (“thalamic glioma”).
|
 DEVELOPMENT AND FUNCTION OF THE CHOROID PLEXUS: The choroid plexus is a dense network of small blood vessels in the ventricular system of the brain. There are four choroid plexuses in the brain: two in the lateral ventricles (lateral choroid plexuses) and one in the third ventricle and in the fourth ventricle (central choroid plexuses).
The ventricular system is made up of four cavities joined by narrow passages to allow the circulation of cerebrospinal fluid. The highest ventricles are the two lateral ventricles deep within the cerebral hemispheres. Each lateral ventricle is structured in a C-shape, reaching from the temporal lobes to the pre-motor sensory cortex. The third ventricle below them is located in the diencephalon (interbrain) between the right and left thalamus. The fourth ventricle between the brainstem and the cerebellum connects with the subarachnoid space (see meninges) and the central canal of the spinal cord. The cerebral aqueduct joins the third and fourth ventricle. The ventricles and cerebrospinal fluid protect the brain and spinal cord from injury.
 This image highlights the four ventricles as they show on a brain CT.
A choroid plexus consists mainly of ependymal cells. The main function of the ependymal cells is the production of cerebrospinal fluid (secretory quality) through the filtration of arterial blood. Cerebrospinal fluid (CSF) drains from the lateral ventricles into the third ventricle further via the cerebral aqueduct into the fourth ventricle. From there the fluid escapes through lateral openings of the fourth ventricle into the subarachnoid space. The ependymal cells of the choroid plexus form a thin layer (ependyma) that covers the inner wall of the ventricles and surrounds the core of the plexus. The ependyma acts as an important filter, known as the blood-cerebrospinal fluid barrier (BCSFB). The blood-cerebrospinal fluid barrier is in addition to the blood-brain barrier (BBB) a dynamic interface to maintain a stable environment for brain cells (neurons). The two barriers restrict the passage of large molecules, including microbes and cancer cells (see “metastatic brain tumors”), into the brain while allowing the entry of water, lipid-soluble substances (oxygen, carbon dioxide), and molecules such as amino acids and glucose. Sugar is nutrition for the brain. Cerebrospinal fluid, also known as cerebrospinal “liquor” (sweet substance), is therefore rich in glucose (the brain consumes 25% of the body’s energy using about 150g of glucose daily).
The ependymal cells of the choroid plexus originate from the endoderm and are therefore controlled from the brainstem. Neuroglial cells that provide support to the ependymal cells are of new mesodermal origin.
 BRAIN LEVEL: In the brainstem, the choroid plexuses have two control centers positioned within the ring form of the brain relays that control the organs of the alimentary canal.
The right lateral choroid plexus and right halves of the central choroid plexuses are controlled from the right side of the brainstem; the left lateral choroid plexus and left halves of the central choroid plexuses are controlled from the left brainstem hemisphere. There is no cross-over correlation from the brain to the organ.
NOTE: The mouth and pharynx, tear glands, Eustachian tubes, thyroid gland, parathyroid glands, pituitary gland, pineal gland, and choroid plexuses share the same brain relays.
BIOLOGICAL CONFLICT: According to its function as the “waterworks of the brain”, the biological conflict linked to the choroid plexuses is “the brain is not moist enough” or “the brain is dry” experienced, figuratively, when one has difficulties thinking (the thoughts don’t flow smoothly) or memorizing. A distressing mental blackout, short-term memory loss (see separation conflict), or learning difficulties could cause such a conflict. Also, considering the correspondence of brainstem-controlled organs to an ingoing (food) morsel and outgoing (feces) morsel, the conflict linked to the right lateral choroid plexus and right halves of the central choroid plexuses is “not being able to let a morsel ‘flow in’”. Accordingly, the conflict linked to the left lateral choroid plexus and left halves of the central choroid plexuses is “not being able to let a morsel ‘flow out’”. Such a “morsel” can relate to anything one desires to “catch” or “get rid of”, including a person (compare with conflicts related to the mouth and pharynx submucosa).
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase ependymal cells of the choroid plexus proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to enhance the production of cerebrospinal fluid. With prolonged conflict activity a compact tumor (secretory type) forms as a result of the continuing cell augmentation. In conventional medicine, this is called a choroid plexus ependymoma. Contrary to a glioma, an ependymoma is a real brain tumor (see also pineal tumor and a pituitary adenoma).
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer required. With the participation of TB bacteria the condition is called ependymoma tuberculosis, typically accompanied by night sweats. During the decomposing process the tumor might bleed into the affected ventricle. The bleeding occurs when the outer wall of the tumor breaks (compare with brain bleeding due to the rupture of a brain cyst).
 After an ependymoma has been decomposed, caverns remain at the site that are eventually filled with calcium, showing as calcium deposits on a brain scan (here in the lateral ventricles).
 This brain CT demonstrates a complete calcification process in the third ventricle (compare with calcification in the pituitary gland and pineal gland).
HYDROCEPHALUS
A hydrocephalus is a condition in which excess cerebrospinal fluid (CSF) accumulates in the cavities of the brain. This occurs when a tumor or a big brain edema compresses one of the ventricles or the cerebral aqueduct. A brain edema in the control center of the kidney parenchyma could lead to a compression of the cerebral aqueduct. Swelling in the brain relays of the lung alveoli (related to a death-fright conflict) can compress the fourth ventricle resulting in the dilation of the entire ventricular system. A healing process (PCL-A) involving the brain relays of the thalamus or myocardium might block the third ventricle from both sides. Brain edemas usually enlarge due to water retention (the SYNDROME) and an active abandonment or existence conflict. The accumulation of CSF and the pressure caused by the fluid buildup increases the size of the ventricles creating an internal hydrocephalus. With an external hydrocephalus the fluid accumulation occurs in the subarachnoid space; if it involves the frontal lobe it is characterized by a prominent forehead developing in infancy.
The enlargement of the head happens when the skull bones are not fully fused, which is the case in fetuses and infants up to the age of two. Unborn children experience existence conflicts and death-fright conflicts because of extreme distress in the womb (see intrauterine conflicts); newborns suffer abandonment conflicts when they are separated from the mother at birth. In adults, the skull cannot expand to accommodate the buildup of cerebrospinal fluids. Subsequent symptoms are headaches, nausea, and drowsiness. Strong, elevated intracranial pressure may result in an elongation of the cerebellar tonsils, the rounded lobes underneath the cerebellar hemispheres; a life-threatening condition occurs when the pressure pushes the tonsils out of the skull (the descent of the cerebellar tonsils is termed “tonsillar herniation”). Lasting increased pressure on the optic nerve cuts off the oxygen supply to the optic nerve, causing it to swell. Swelling of the optic nerve at the point where the nerve joins the eye is called a papilledema (compare with excavation papillae due to permanent elevated intraocular pressure). Damage to the optic nerve from papilledema can result in visual field loss. With hydrocephalus, a weakening of the nerves that control eye movement creates eye misalignment (see strabismus). Symptoms such as weakness of the legs, epileptic seizures, or speech problems, however, are not brought on by a hydrocephalus, as claimed, but relate to specific Biological Special Programs.
 This brain CT shows an expansion of the lateral ventricles (internal hydrocephalus) caused by an accumulation of cerebrospinal fluid.
 A compression of the fourth ventricle can be the result of an acute fear of life conflict leading to a hydrocephalus after the conflict has been resolved. In this example, the corresponding Hamer Focus reaches over the entire brainstem. Excessive noise during pregnancy, for example, could trigger the panic in the unborn (see intrauterine conflicts).
|
 DEVELOPMENT AND FUNCTION OF THE MYELIN SHEATH: The myelin sheath forms an insulating layer around nerves, including nerves in the brain and spinal cord. Each nerve cell or neuron consists of a cell body with a nucleus (which contains DNA) and dendrites (nerve endings) projecting out from the cell body to receive signals from other neurons. The axon is an extension that differs from the dendrites insofar as it carries impulses away from neurons, sometimes over a considerable distance. Longer axons are covered with a myelin sheath. The function of the myelin sheath is to speed the electrical transmission along the nerve cells. The myelin sheath enveloping motor neurons aids in the conduction of nerve impulses to the muscles; sensory neurons communicate sensory stimuli such as touch. Myelinated neurons are therefore typically found in the peripheral nerves.
Myelin originates from Schwann cells, which are specialized glial cells. Glial cells (also called neuroglia) provide support and protection for neurons in the brain and spinal cord (central nervous system). Schwann cells, on the other hand, are found in the peripheral nervous system (outside of the brain) where they form the myelin sheath around nerve cells. In humans, myelination begins in the fourteenth week of the fetal development. Like glia, myelin consists for the most part of connective tissue. The myelin sheath derives therefore also from the new mesoderm.
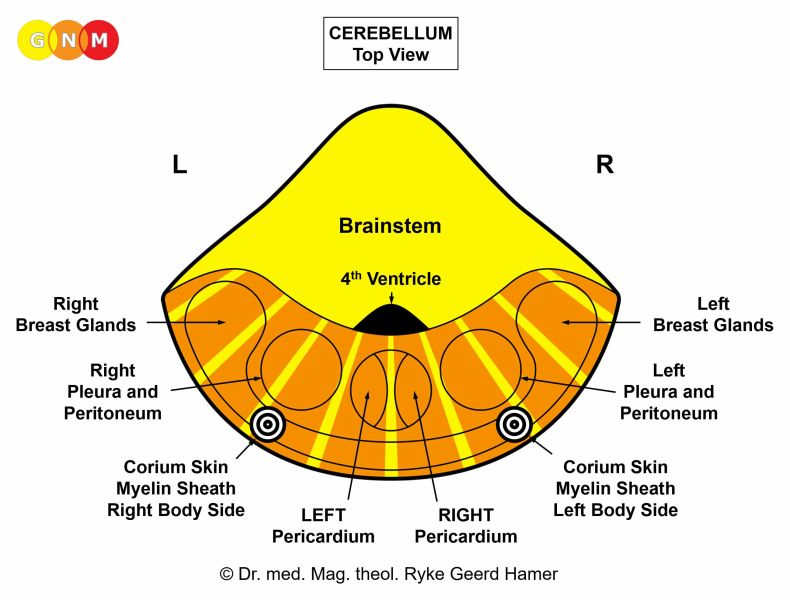 BRAIN LEVEL: Exception: Even though the myelin sheath is of new mesodermal origin, it is controlled from the cerebellum rather than from the cerebral medulla.
The myelin sheath on the right side of the body is controlled from the left side of the brain; the myelin sheath on the left side of the body is controlled from the right brain hemisphere. There is a cross-over correlation from the brain to the body.
NOTE: The myelin sheath is controlled from the same brain relay as the corium skin (see also eyelid glands).
BIOLOGICAL CONFLICT: The biological conflict linked to the myelin sheath is a touch conflict of not wanting to be touched because the touch is experienced as painful, unpleasant or unwanted (compare with separation conflict related to the outer skin). The fear of being touched (physical abuse, sexual abuse) can already evoke the conflict. The myelin sheath also responds to a pain conflict triggered by acute pain due to an injury, fall, or hit. Severe pain, for example, bone pain can also activate the Biological Special Program.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase the myelin sheath thickens through cell proliferation forming a neurofibroma beneath or on the skin (like a melanoma, a neurofibroma is an archaic form of defense). The size of the nodule(s) is determined by the intensity of the conflict. The biological purpose of the cell increase is to block the peripheral sensory stimuli from being transmitted to the brain. The extra tissue absorbs the unwanted touch or pain. Symptom: a loss or decreased sensitivity to touch at the affected area (see also hyposensitivity involving the epidermis or the periosteum).
 The appearance of a neurofibroma under the skin (subcutaneous neurofibroma) is similar to that of a lipoma involving the fat tissue.
When situated immediately beneath the skin, neurofibromas are readily movable.
 Multiple neurofibromas beneath or on the skin (cutaneous neurofibroma) are termed neurofibromatosis type 1 (NF1) or von Recklinghausen’s disease. Café-au-lait pigmentations (coffee-colored patches on the skin) classified as symptoms of NF1 are, based on GNM, related to the epidermis rather than to the nerve sheath. The fact that café-au-lait spots are observed in the majority of people with NF1 is an indication that the two Biological Programs (separation conflict and touch conflict) often run concurrently.
HEALING PHASE: Following the principle of organs deriving from the new mesoderm (“surplus group”), the neurofibroma(s) stay in place. With the completion of the healing phase the sensitivity returns to normal.
|
 DEVELOPMENT AND FUNCTION OF THE MENINGES: The meninges are the three thin membranes that envelop the brain and the spinal cord. The primary function of the meninges is to protect the central nervous system. The meninges consist of the pia mater (inner meninges), which follows closely the contours and folds (gyri and sulci) of the brain, the arachnoid mater, and the dura mater (outer meninges). The space between the pia mater and arachnoid mater (subarachnoid space) is filled with cerebrospinal fluid (see choroid plexus). The outer surface of the skull bones is covered by the periosteum and the skin (corium skin and epidermis). The pia mater (“soft mother”) is a delicate membrane endowed with many blood vessels that nourish the brain. The dura mater (“tough mother”) is composed of dense fibrous tissue with a periosteal layer close to the inner surface of the skull. The dura mater, arachnoid mater, and pia mater originate from the new mesoderm and are controlled from the cerebral medulla. The periosteal nerves of the dura mater are controlled from the pre-motor sensory cortex; the control center is located close to the brain relays of the pharyngeal ducts and thyroid ducts at the front of the cortex.
Meningitis
Conventional medicine argues that inflammations of the meninges are the result of “infections” with viruses, bacteria, or fungi that allegedly migrate via the bloodstream to the brain and spinal cord. Any such claim is highly questionable because the blood-brain barrier that separates the circulating blood from the cerebrospinal fluid allows only water, lipid-soluble substances, and molecules (glucose and amino acids) into the brain. This strictly excludes the entry of microbes that are supposedly transmitted to humans by “infected” ticks leading to meningoencephalitis, an inflammation of the meninges and the brain (see also Lyme disease-associated meningitis). This means that under no circumstances are bacteria able to reach the meninges via the bloodstream. The assertion that bacterial meningitis is “highly contagious” is therefore unfounded.
The only way bacteria find their way into the central nervous system is when the spinal cord gets punctured. During the puncture, a hollow needle is inserted into the subarachnoid space to collect cerebrospinal fluid. In today’s medicine, a lumbar puncture, colloquially called a spinal tap, is a common diagnostic procedure to confirm or exclude meningitis.
Based on GNM, meningitis occurs
In PCL-B, after the brain edema has been expelled, glial cells proliferate at the site to complete the healing process. In conventional medicine, this is often diagnosed as a meningioma, believed to be a “brain tumor” arising from meningothelial cells in the meninges.
Depending on the location of the edema signs and symptoms of meningitis range from flu-like symptoms and pneumonia to neck stiffness, muscle paralysis, epileptic seizures or skin rashes. The severe headaches are caused by the swelling of the brain edema as well as by the inflammation (compare with headaches in the course of any Biological Special Program and migraine headaches). The inflammation is typically accompanied by high fever. With sudden water retention due to an active abandonment or existence conflict (the SYNDROME) the brain edema increases quickly in size and the meningitis symptoms occur within a few days.
Meningitis most commonly affects children under five years of age, particularly babies under the age of one. Brain damage associated with meningitis is unlikely caused by a brain edema (wrongly assumed to be a swelling of the meninges) but rather by vaccines containing neurotoxins such as formaldehyde, aluminum phosphate, or thimerosal that bypass the blood-brain barrier resulting in potentially serious neurological disorders, without a DHS!
If several healing phases happen to occur at the same time, the swellings in the brain can lead to an inflammation of the brain, termed encephalitis. Like meningitis, this has nothing to do with an “infection”. Encephalitis might also develop after a brain injury or brain surgery. A swelling in the area of the spine (see osteosarcoma) can put pressure on the meninges of the spinal cord leading to myelitis. A large swelling might cause serious complications.
| ||||||||||||||
