Teeth and Jaw
 DEVELOPMENT AND FUNCTION OF THE DENTIN AND THE JAW BONES: A human adult has 32 teeth, 16 in the upper jaw and 16 in the lower jaw. Each tooth consists of a crown (above the gum line) covered by enamel and a root (below the gum line). The tooth is for the most part made of dentin. Its calcified structure is denser than that of bones, which allows withstanding the stress of biting and grinding. The roots of the teeth reach into the upper or lower jaw bones. The root canals extend from the tip of the root into the pulp chamber, located in the center of the tooth. The pulp contains blood vessels that nourish the tooth and nerves that provide sensitivity to heat, cold, pain, and pressure. The pulp cells, called odontoblasts, are capable of producing dentin (similar to bone-building osteoblasts ). The pulp is quasi the “bone marrow” of the tooth. The periodontium (also termed odontoperiosteum) surrounding the dentin provides support to the teeth (equivalent to the periosteum covering the bones). The gums (see mouth submucosa and mouth surface mucosa) or gingiva lies over the jaw bones and hugs the tooth tightly at the neck. The jaw is a pair of bones that forms the framework of the mouth. It consists of the maxilla (fixed upper jaw bone), the mandible (movable lower jaw bone), and the temporomandibular joint (TMJ). The function of the jaw is its use for biting and chewing (see also jaw muscles). The dentin and jaw bones originate from the new mesoderm and are therefore controlled from the cerebral medulla.
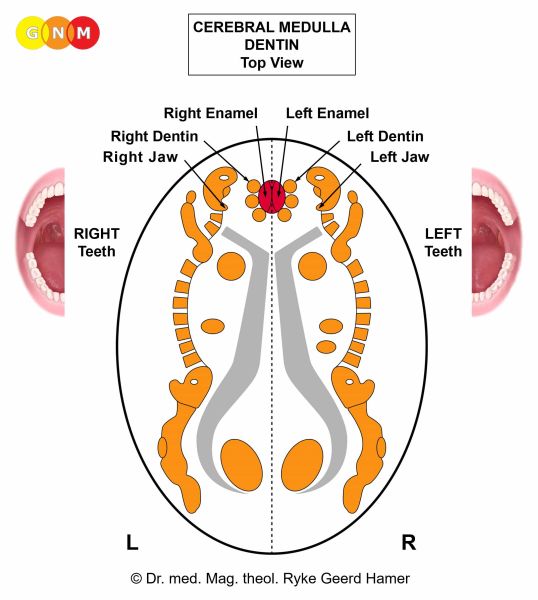 BRAIN LEVEL: In the cerebral medulla, the dentin of the right teeth and the right jaw bones are controlled from the left side of the brain; the dentin of the left teeth and the left jaw bones are controlled from the right cerebral hemisphere (paramedial). Hence, there is a cross-over correlation from the brain to the organ.
BIOLOGICAL CONFLICT: The biological conflict linked to the dentin is not being able to bite, either literally (being unable or having difficulties manipulating food) or figuratively, in the sense of not being able to “bite” or “snap at” an opponent, because the individual is in a weaker position (compare with bite conflict related to the enamel and the jaw muscles). For example, physically weaker (a child vis-à-vis a bigger child or an adult, a woman vis-à-vis a man, a small dog vis-à-vis a big dog), in a weaker position at the workplace (an employee vis-à-vis the boss or a colleague in a higher position), at school (a student vis-à-vis a teacher, a teacher vis-à-vis the principle), within the family (a child vis-à-vis a parent or an older sibling; a new spouse or partner vis-à-vis a stepchild), or in a weaker position vis-à-vis an authority (government official, policeman, doctor, judge, bank manager). Discrimination, political oppression, abuse (physical, sexual, verbal), punishments, restrictions, provocations, or being scolded create situations that could trigger a bite conflict. The conflict is experienced as not being able to fight back or fight someone off in defense (“showing one’s teeth”). Verbal fights and constant arguing with a family member are classic bite conflicts. The bite conflict related to the dental bone is a type of self-devaluation conflict (see bones and joints). Unattractive teeth, because of poor dental hygiene, can therefore also cause a dentin-related conflict. The bite conflict associated with the jaw bones is perceived as more intense.
Location: Which teeth are affected by the bite conflict is determined by the individual perception of the conflict situation in correspondence to the specific function of the teeth.
 The incisors (front teeth) are used for biting and cutting food. The related bite conflict: not being able to bite, snap at someone, or show one’s teeth.
The canines (at the corner) are used for gripping and tearing food. The related bite conflict: not being able to snatch a person.
The molars (at the back) are used for crushing and chewing food. The related bite conflict: not being able to crunch or grind an opponent (“chewing him up and spitting him out”).
CONFLICT-ACTIVE PHASE: loss of dentin causing holes (cavities) in the tooth. Since dentin cavities are painless (contrary to cavities in the enamel) they are usually only detected through an X-ray. If, however, a cavity progresses to the pulp, the exposure of the pulp causes a painful sensitivity to hot, cold, sweet, or sour foods and drinks. Excessive dentine loss due to lasting conflict activity destroys the internal structures of the tooth with the result that the tooth breaks. Without blood supply to the pulp, the tooth starts to rot from the inside.
 Here we see the impact of a bite conflict in the control center of the dentin (view the GNM diagram). The Hamer Focus reaches over both brain hemispheres (central conflict). This reveals that the person associated the conflict with his/her mother/child and partner, for example, with both parents (father and mother), causing cavities in the right and left teeth (compare with impact of a central conflict in the enamel relay).
If the jaw is affected, the jaw bone decalcifies (osteolysis). With prolonged conflict activity, the neck of the tooth gets visibly longer, the gums recede and the tooth becomes loose and unstable. Consequently, the gums tear easily causing gum bleeding (gum diseases such as a gum abscess or gingivitis relate to the mouth submucosa and mouth surface mucosa). The degeneration of the periodontal structure is called periodontosis. There is a risk that the tooth falls out.
HEALING PHASE: In the healing phase, the cavities in the tooth are refilled with dentin callus produced by odontoblasts in the pulp (similar to the reconstruction of bones with callus produced by bone-building osteoblasts). The soft callus eventually hardens.
 In the jaw, the soft bone callus makes the tooth or teeth shift easily. Dental braces designed to align and straighten the teeth work therefore best during that period.
If a tooth cavity has an external opening (see tooth fistula) the callus finds its way into the mouth. Combined with food remnants and saliva, the sticky substance adheres to the surface of the teeth contributing to the formation of tartar, a form of hardened dental plaque. Contrary to the common belief, dental plaque does not cause cavities. Plaque is also believed to cause gingivitis, an inflammation of the gums. This theory, however, cannot explain why cavities or gingivitis occur on the right or left side of the mouth, why cavities develop in a very specific tooth, why they affect the front teeth or molars, or why the “caries” occurs in the dentin or in the tooth enamel. German New Medicine offers insights into the cause of “tooth diseases” that will fundamentally change dental medicine as we know it.
During the replenishing process, the periodontium covering the tooth stretches due to the swelling. This can cause a severe toothache since the squamous epithelial layer covering the periodontium is endowed with highly sensitive nerves (compare with dental pain involving the enamel). If the cavity formed inside the tooth rather than towards the border, the swelling might press on the pulp. In this case, the pain could be excruciating. Prolonged pressure on the pulp (hanging healing) might damage the tooth’s nerves (the pulp can also become damaged through repeated dental work on a tooth or large fillings). At that point, the standard treatment is a root canal or an extraction of the tooth.
The root canal procedure entails removing the entire contents of the pulp and filling the cavity with a plastic material called gutta-percha. There is more to it than that: The filling also contains formaldehyde and arsenic!
What is left after a root canal is a dead and toxic tooth! The theory that a root-canaled tooth bears the risk of developing cancer or of having a heart attack, as originally proposed by Dr. Weston A. Price (in 1922), is, based on the Five Biological Laws, highly doubtful. From a GNM point of view, a root canal should be avoided at all costs. In exceptional cases, the affected tooth might have to be extracted and replaced.
Bacteria, provided they are available, assist the reconstruction of the tooth. The microbial activity causes an abscessed tooth with an accumulation of callus and pus inside the tooth (compare with gum abscess). The pain of the tooth abscess is due to the buildup of pressure inside the tooth. If, however, the cavity has created an external opening, called a tooth fistula, the pus will leak out and drain the abscess on its own.
 The swelling around the tooth (see picture) results from to the edema (fluid accumulation) in the healing area. With water retention because of the SYNDROME, the swelling becomes considerably larger, noticeable as facial swelling.
In the jaw, the recalcification that occurs during the healing phase is also accompanied by swelling and pain, caused by the stretching of the periosteal layer covering the jaw bones. A large swelling is usually diagnosed as jaw cancer (see bone cancer). Pain in the temporomandibular joint is referred to as TMJ syndrome.
|
 DEVELOPMENT AND FUNCTION OF THE TOOTH ENAMEL: The enamel covers the crown of the tooth above the gums. It is composed of large amounts of minerals (more than contained in dentin) accounting for its strength to protect the teeth from daily use such as chewing, biting, and grinding. Like the neural network of the periosteum, the enamel has two layers: an inner layer close to the dentin, and an outer, visible layer. The lining of the periodontium (odontoperiosteum) on top of the dental bone consists of squamous epithelium. The outer layer of the enamel is hardened squamous epithelium. The enamel originates from the ectoderm and is therefore controlled from the cerebral cortex.
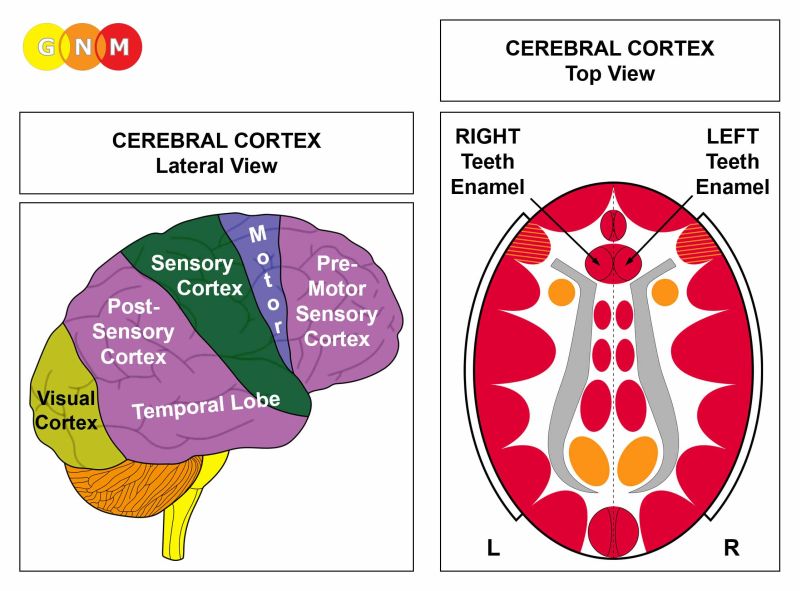 BRAIN LEVEL: The tooth enamel is controlled from the pre-motor sensory cortex (part of the cerebral cortex). The enamel of the right teeth is controlled from the left side of the cortex; the enamel of the left teeth is controlled from the right cortical hemisphere. Hence, there is a cross-over correlation from the brain to the organ.
BIOLOGICAL CONFLICT: While the tooth dentin relates to “not being able to bite”, the biological conflict linked to the tooth enamel is not being allowed to bite either literally (a big dog is not allowed to bite a small dog because his master is holding him back; not being allowed to “bite into” one’s favorite food – compare with oral conflict) or figuratively, in the sense that the individual is prevented from “biting” or “snapping” at someone. More precisely, the person could “bite” because he/she is stronger or in a higher position or rank but because of rules (rules of etiquette or political correctness) or for ethical reasons is not permitted to “snap back”. Refraining from saying something (keeping from snapping at someone) in order not to hurt the person could also cause a bite conflict. In addition, the bite conflict associated with the enamel corresponds to “not being allowed or not being able to hold on to something” (similar to a mother cat holding her kitten by gripping its neck with her teeth). It is a type of separation conflict (see periosteum).
Location: Which teeth are affected by the bite conflict is determined by the individual perception of the conflict situation in correspondence to the specific function of the teeth.
The incisors (front teeth) are used for biting and cutting food. The related bite conflict: not being allowed to bite, snap at someone, or show one’s teeth.
The canines (at the corner) are used for gripping and tearing food. The related bite conflict: not being allowed to snatch a person.
The molars (at the back) are used for crushing and chewing food. The related bite conflict: not being allowed to crunch or grind an opponent (“chewing him up and spitting him out”).
CONFLICT-ACTIVE PHASE: ulceration of the enamel causing cavities in the affected tooth or teeth (compare with cavities in the dentin). The biological purpose of the enamel loss is to make the tooth blunt in order to be unable to bite (since it is not allowed). The pain (“tooth rheumatism”) is similar to the rheumatic pain involving the periosteal nerves. Like the neural network covering the periosteum, the periodontium (odontoperiosteum) lying on top of the dental bone is supplied by highly sensitive nerves (compare with toothache in the healing phase of the dentin caused by the stretching of the periodontium). When the enamel is lost, there is also a heat and cold sensitivity.
With prolonged conflict activity the decayed tooth shows black spots or becomes entirely black, depending on the intensity and duration of the conflict. Tooth decay, whether it occurs in the dentin or in the enamel, is unrelated to sugar in foods or liquids.
 Note in this picture that the decay of the enamel only involves the incisors of the left teeth. If the person is left-handed, this reveals that the bite conflict was associated with a partner.
 This picture shows advanced enamel cavities restricted to the right and left incisors. This indicates that the bite conflict is related to the person’s mother/child and partner.
 Accordingly, the Hamer Focus showing on a CT scan in the enamel relay (view the GNM diagram) reaches over both brain hemispheres (central conflict) – compare with impact of a central conflict in the dentin relay.
HEALING PHASE: During the healing phase the enamel tissue is replenished (contrary to the standard view). The restoration process is, however very slow, even without conflict relapses. After the repair, the affected area of the tooth or teeth will remain darker.
|
 DEVELOPMENT AND FUNCTION OF THE JAW MUSCLES: The jaw muscles, or muscles of mastication, are a group of muscles associated with the movements of the jaw (temporomandibular joint), explicitly, with the ability to open and close the mouth, bite, and chew food. The masseter muscle is the primary chewing muscle. It covers the sides of the jaw just behind the cheeks. It is the main muscle that allows clenching the jaw and grinding the teeth; it is also used to control the jaw movement during speech. The jaw muscles consist of striated muscles, originate from the new mesoderm, and are controlled from the cerebral medulla and the motor cortex.
 BRAIN LEVEL: The jaw muscles have two control centers in the cerebrum. The trophic function of the muscles, responsible for the nutrition of the tissue, is controlled from the cerebral medulla; the movement of the jaw muscles is controlled from the motor cortex (part of the cerebral cortex). The right jaw muscles are controlled from the left side of the cerebrum; the left jaw muscles are controlled from the right cerebral hemisphere. Hence, there is a cross-over correlation from the brain to the organ (see GNM diagram showing the motor homunculus).
BIOLOGICAL CONFLICT: The biological conflict linked to the jaw muscles is a self-devaluation conflict of not being able or not being allowed to “bite” an opponent (a competitor, colleague, classmate, teacher, family member, relative, neighbor) or to “snap up” something that one desires (see also bite conflict related to the dentin and enamel) or, figuratively, not being able or not being allowed to say something or express oneself. The conflict can also be experienced in real terms as in “not being able to open the mouth widely enough or ‘properly’” (for instance, during a dental procedure) or “not wanting to open the mouth”. It is a type of localized motor conflict (“not being able to move the jaw”).
CONFLICT-ACTIVE PHASE: cell loss (necrosis) of jaw muscle tissue (controlled from the cerebral medulla) and, proportional to the degree of conflict activity, increasing paralysis of the jaw muscles (controlled from the motor cortex) affecting the ability to move the jaw (termed TMJD-Temporomandibular Joint Dysfunction). Difficulties opening or closing the mouth, called lockjaw, are also associated with the temporomandibular joint (TMJ).
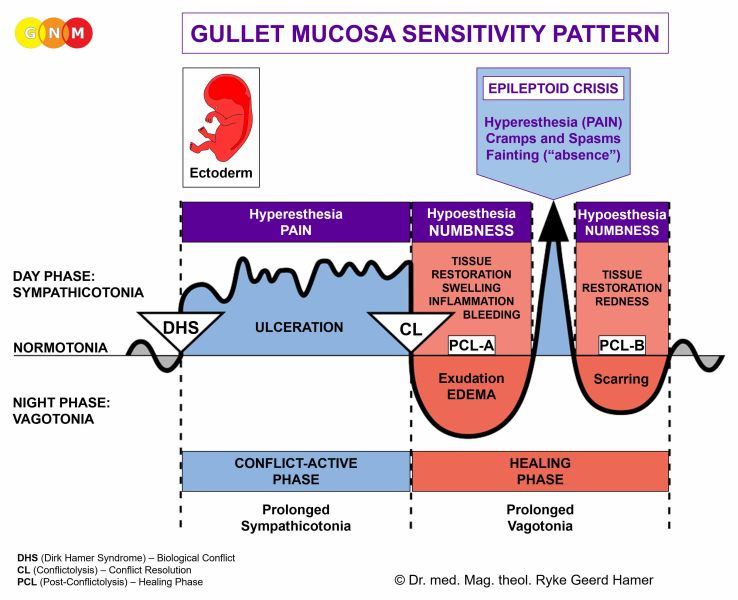
HEALING PHASE: In the healing phase, the jaw muscles are reconstructed; the paralysis reaches into PCL-A. The Epileptoid Crisis presents as spasms of the jaw muscles. Bruxism, excessive grinding of the teeth and/or clenching of the jaw, typically occurs during sleep. After the Epi-Crisis, in PCL-B, the function of the jaw muscles returns to normal.
| ||||||||||||||||