Thyroid
 DEVELOPMENT AND FUNCTION OF THE THYROID GLAND: The thyroid gland is situated at the front of the lower neck below the larynx with one lobe on each side of the trachea. Originally, the thyroid gland was located in the oropharynx from where it descended to its final position, taking a path through the tongue and the neck. This connection is known as the thyroglossal duct. The primary function of the thyroid is the production of thyroxine (secretory quality), a hormone that regulates the rate in which nutrients are converted into energy (see pituitary gland, TSH-thyroid stimulating hormone). Initially, the thyroid was an exocrine gland excreting hormones into the ingoing and outgoing section of the intestine to facilitate the ingestion of food and the elimination of feces. After the gullet had broken open, the thyroid became an endocrine gland releasing thyroxine directly into the bloodstream. The thyroid gland consists of intestinal cylinder epithelium, originates from the endoderm and is therefore controlled from the brainstem.
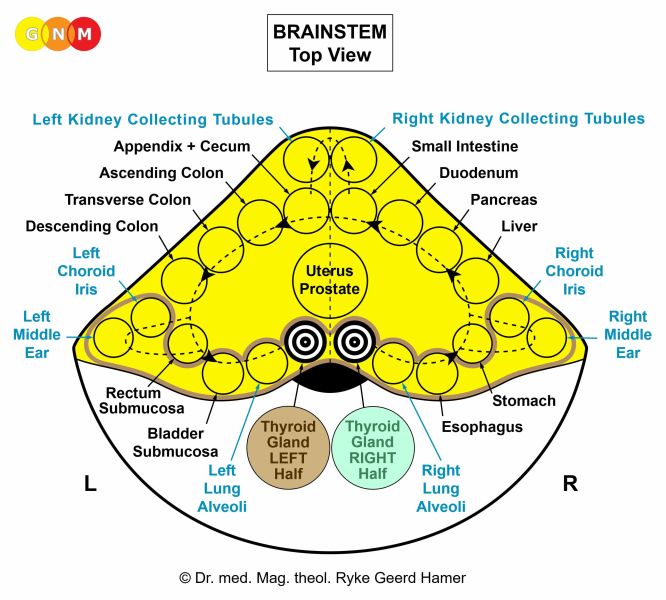 BRAIN LEVEL: In the brainstem, the thyroid gland has two control centers that are orderly positioned within the ring form of the brain relays that control the organs of the alimentary canal.
The right half of the thyroid gland is controlled from the right side of the brainstem; the left half is controlled from the left brainstem hemisphere. There is no cross-over correlation from the brain to the organ.
NOTE: The mouth and pharynx, tear glands, Eustachian tubes, thyroid gland, parathyroid glands, pituitary gland, pineal gland, and choroid plexuses share the same brain relays.
BIOLOGICAL CONFLICT: Consistent with its role in digestion, the biological conflict linked to the thyroid gland is a “morsel conflict” (compare with “morsel conflict” related to the parathyroid glands, mouth and pharynx, stomach, duodenum, pancreas gland, small intestine, and colon).
RIGHT HALF OF THE THYROID GLAND
 Equivalent to the right half of the mouth and pharynx, the conflict linked to the right lobe of the thyroid relates to an “ingoing morsel” and to “not being fast enough to catch a morsel”. Such a “morsel” concerns, for example, a job, a position, a promotion, a contract, a business, or a purchase one strongly desires but is too slow to “grab”. The expected “morsel” could also relate to a person one is too slow to “catch” or “get a hold of”.
LEFT HALF OF THE THYROID GLAND
 Equivalent to the left half of the mouth and pharynx, the conflict linked to the left lobe of the thyroid relates to an “outgoing morsel” and to “not being fast enough to eliminate a morsel” (originally, the feces morsel). This could be a term paper, any kind of goods, foul stocks or a person (tenant, employee, business partner) one was too slow to “get rid of”. An apology or a proposal that was expressed too late can also evoke this type of “morsel” conflict.
People who are driven to “get things done”, who have professions and activities that involve competition (business managers, sales agents, vendors, athletes and sports competitors), who are under deadline pressure (journalists, manufacturers) or constant pressure to “keep up” (working two jobs, single mothers) are more susceptible to experience the conflict. Children and adolescents suffer thyroid-conflicts when they are pushed by a parent, teacher, or coach (“You are too slow!”).
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase thyroid gland cells proliferate proportionally to the intensity of the conflict. The biological purpose of the cell increase is to improve the secretion of thyroxine so that the individual becomes faster to catch the desired morsel (right half of the thyroid) or to get rid of an undesired morsel (left half of the thyroid). This causes an overactive thyroid or hyperthyroidism. Because of the enhanced thyroxine production, persons with an overactive thyroid are often overexcited, nervous, irritable, and have trouble sleeping. High blood pressure is typically isolated to systolic hypertension (compare with hypertension related to the right myocardium and the kidney parenchyma). The nodule that appears during the conflict-active phase is generally referred to as a “hot nodule” (compare with “cold nodule” related to the thyroid ducts).
 With persistent conflict activity, the growth (secretory type) created by the continuing cell augmentation forms a hard struma, or goiter (compare with euthyroid struma related to the thyroid ducts). The enlargement of the thyroid could cause breathing difficulties due to the pressure on the trachea. A large swelling with profuse cell proliferation might be diagnosed as a thyroid cancer.
 This CT scan highlights the area in the brainstem from where the left thyroid gland is controlled (view the GNM diagram). The sharp ring configuration of the Hamer Focus indicates conflict activity, hence, an overactive thyroid.
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. Healing symptoms are pain due to the swelling, difficulties breathing and swallowing, and night sweats. If the healing process is accompanied by an inflammation, this causes thyroiditis.
With the completion of the healing phase the thyroxine level returns to normal. However, with a hanging healing, that is, when healing is continually interrupted by conflict relapses, the prolonged decomposing process results in a loss of thyroid gland tissue causing a chronic underactive thyroid, or hypothyroidism, also termed Hashimoto’s disease. It is a wide-spread belief that hypothyroidism is caused by iodine deficiency. This theory, however, cannot explain why the right or left thyroid lobe is affected or both. Symptoms of an underactive thyroid are fatigue and low energy, since the insufficient production of thyroxine slows down the body’s metabolism (see also healing phase of thyroid ducts). In this case, supplementing thyroxine is advisable.
NOTE: Hypothyroidism is always preceded by hyperthyroidism!
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells in the thyroid gland cannot be broken down. Consequently, the growth or goiter stays maintaining the overproduction of thyroxine with lasting hyperthyroidism, even though the conflict has been resolved (see also parathyroid glands, pancreas gland, adrenal gland, prostate gland). To normalize the thyroxine production, surgery might have to be considered.
|
 DEVELOPMENT AND FUNCTION OF THE PARATHYROID GLANDS: The parathyroid glands are two pairs of small glands located on the back side of the thyroid gland. Their main function is to secrete a hormone (PTH-parathyroid hormone) that helps maintain the proper level of calcium (secretory quality), a mineral essential for muscle contraction. Like the thyroid gland, the parathyroid glands were originally exocrine glands that excreted into the intestine. Today, they are endocrine glands that release their hormones directly into the bloodstream. The parathyroid glands consist of intestinal cylinder epithelium, originate from the endoderm and are therefore controlled from the brainstem.
 BRAIN LEVEL: In the brainstem, the parathyroid glands have two control centers that are orderly positioned within the ring form of the brain relays that control the organs of the alimentary canal.
The right parathyroid glands are controlled from the right side of the brainstem; the left parathyroid glands are controlled from the left brainstem hemisphere. There is no cross-over correlation from the brain to the organ.
NOTE: The mouth and pharynx, tear glands, Eustachian tubes, thyroid gland, parathyroid glands, pituitary gland, pineal gland, and choroid plexuses share the same brain relays.
BIOLOGICAL CONFLICT: According to the function of the parathyroid glands, the corresponding biological conflict is a “morsel conflict” (compare with “morsel conflict” related to the thyroid gland, mouth and pharynx, stomach, duodenum, pancreas gland, small intestine, and colon).
RIGHT PARATHYROID GLANDS: Equivalent to the right half of the mouth and pharynx, the conflict linked to the right parathyroid glands relates to an “ingoing morsel” and to “not being able to catch a morsel” because of a low calcium level limiting the muscle contraction required to ingest a food morsel.
LEFT PARATHYROID GLANDS: Equivalent to the left half of the mouth and pharynx, the conflict linked to the left parathyroid glands relate to an “outgoing morsel” and to “not being able to eliminate a morsel” because of a low calcium level limiting the muscle contraction required to eliminate a morsel.
CONFLICT-ACTIVE PHASE: Starting with the DHS, during the conflict-active phase cells in the parathyroid glands proliferate causing an overproduction of PTH or hyperparathyroidism with the biological purpose to supply the organism with more calcium to improve the muscular contraction so that the morsel can be better absorbed (right glands) or eliminated (left glands). Consequently, the calcium level in the blood increases causing hypercalcemia (compare with hypercalcemia related to the bones). In conventional medicine, a large growth in the parathyroid glands might be diagnosed as a parathyroid cancer.
HEALING PHASE: Following the conflict resolution (CL), fungi or mycobacteria such as TB bacteria remove the cells that are no longer needed. This process is accompanied by night sweats. With the completion of the healing phase the PTH level returns to normal. However, with a hanging healing, when healing is continually interrupted by conflict relapses, the prolonged bacterial activity leads to a loss of parathyroid gland tissue causing chronic hypoparathyroidism with constant low calcium levels. In this case, supplementation is advisable.
NOTE: Hypoparathyroidism is always preceded by hyperparathyroidism!
If the required microbes are not available upon the resolution of the conflict, because they were destroyed through an overuse of antibiotics, the additional cells cannot be broken down causing lasting hyperparathyroidism (see also thyroid gland, pancreas gland, adrenal gland, prostate gland). To normalize the PTH production, surgery might have to be considered.
|
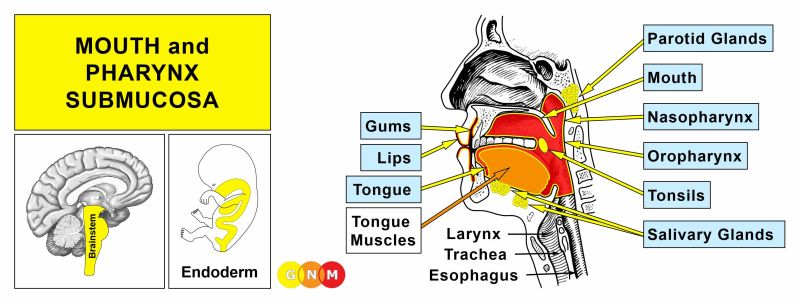
 DEVELOPMENT AND FUNCTION OF THE THYROID DUCTS: The original function of the thyroid ducts was to carry hormones produced in the thyroid gland into the ingoing and outgoing section of the intestine to aid the metabolism of food and the disposal of feces. After the rupture of the gullet, the external openings into the primordial intestine closed and the thyroid became an endocrine gland. Today, the remnants of the thyroid ducts deliver thyroxine directly into the bloodstream. The lining of the thyroid ducts consist of squamous epithelium, originate from the ectoderm and are, therefore, controlled from the cerebral cortex.
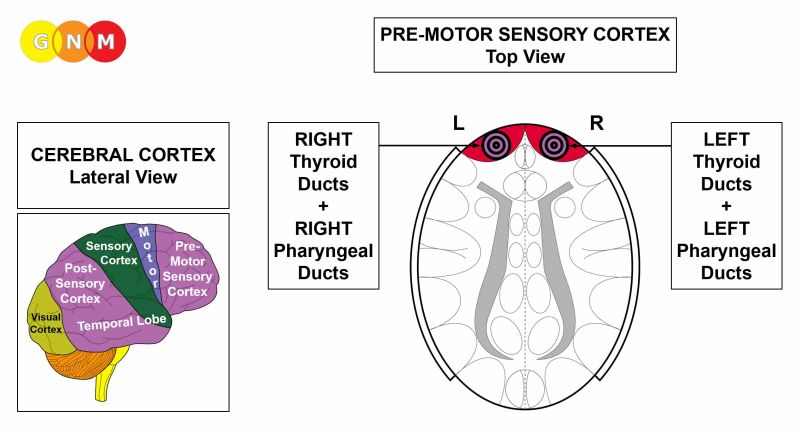 BRAIN LEVEL: The epithelial lining of the thyroid ducts is controlled from the pre-motor sensory cortex (part of the cerebral cortex). The left thyroid ducts are controlled from the right side of the cerebral cortex; the right thyroid ducts are controlled from the left cortical hemisphere (frontal). Hence, there is a cross-over correlation from the brain to the organ.
NOTE: The thyroid ducts and pharyngeal ducts share the same brain relays. The DHS affects either one of the tissues or both, depending on the intensity of the conflict.
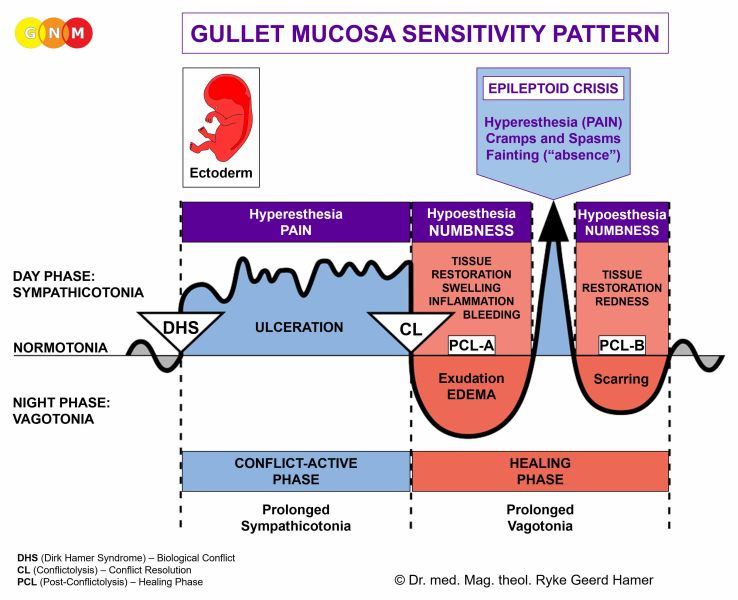
BIOLOGICAL CONFLICT: The biological conflict linked to the thyroid ducts is a female powerless conflict or male frontal-fear conflict, depending on a person’s gender, laterality, and hormone status (see also Frontal Constellation). A powerless conflict is experienced as feeling helpless (“there is nothing I can do about this”, “my hands are tied”) or of not being in control of a situation. Generally speaking, the conflict relates to any kind of imposition, external control or decision made over one’s head.
CONFLICT-ACTIVE PHASE: ulceration in the lining of the affected thyroid duct proportional to the degree and duration of conflict activity. The biological purpose of the cell loss is to widen the duct to supply the organism with more thyroxine; this provides the individual with more energy to resolve the conflict. Symptoms: mild to severe pain, depending on the intensity of the conflict. Since the lumen of the thyroid duct enlarges, the thyroxine level rises slightly during the conflict-active phase. This, however, must not be confused with hyperthyroidism because the thyroxine production in the thyroid gland is unchanged.
HEALING PHASE: During the first part of the healing phase (PCL-A) the tissue loss is replenished through cell proliferation with swelling due to the edema (fluid accumulation). In conventional medicine, the cell mitosis is often diagnosed as a papillary thyroid cancer or papillary carcinoma.
When the swelling occludes a thyroid duct less thyroxine enters the bloodstream, even though the thyroid gland produces the hormone in sufficient amount. According to Dr. Hamer, the decreased supply of the body with thyroxine is never as severe as with hypothyroidism and a chronic reduction of thyroxine-producing cells.
Since the thyroid ducts have no external opening, a cyst forms as a result of the back-up of fluid in the affected duct. The growth is commonly referred to as a “cold nodule” (compare with “hot nodule” related to the thyroid gland). A large thyroid cyst is called a euthyroid struma, or goiter (compare with goiter related to the thyroid gland).
Thyroid cysts are located towards the middle (median) on the right or left side of the neck (compare with cysts in the pharyngeal ducts located laterally). If there are no conflict relapses, the swelling recedes in the course of the healing process. However, with a hanging healing the cyst stays until healing is completed.
 Thyroglossal cysts develop in the thyroglossal duct that connects the thyroid gland with the base of the tongue.
 This brain CT presents a Hamer Focus on the right side of the cerebral cortex, precisely, in the area from where the left thyroid ducts and thyroglossal duct are controlled (view the GNM diagram). The small fluid accumulation, showing as dark, indicates the beginning of PCL-A.
 A thyroid fistula is an external opening of a thyroid duct caused by the rupture of a thyroid cyst (euthyroid struma) with fluids emptying outwards. A thyroid cyst can break, for example, when large amounts of water are retained in the cyst due to the SYNDROME or as a result of continuous conflict relapses that prolong the healing process. Yet, a fistula is only created when the right thyroid ducts are affected since they are located closer to the skin. This explains why a thyroid fistula always forms on the right side of the neck.
 In the brain, the right thyroid ducts, where the fistula occurs, are controlled from the left cortical hemisphere exactly opposite the brain relay of the left thyroid ducts and the perianal ducts. Here is why: Originally, before the gullet broke open, the thyroid was an exocrine gland that released thyroxine into both sections of the intestine. The right thyroid ducts (controlled from the left side of the brain) excreted into the ingoing section (today’s mouth and pharynx, esophagus, stomach and duodenum, small intestine) to aid the digestion of food; the left thyroid ducts (controlled from the right side of the brain) excreted into the outgoing section (today’s rectum) to accelerate the disposal of feces. However, when the gullet ruptured, parts of the left thyroid ducts remained in the rectum. These residues are today’s perianal ducts (see perianal fistula). The close vicinity of the brain control centers of the thyroid ducts and perianal ducts represents the rupture of the gullet on the cerebral level.
| |||||||||||||||||||||||||||||||||||||||||||||||||
{kind=link}